
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington D. C. 20549
FORM 10-K
|
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended June 30, 2020
or
|
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from
Commission file number 001-37823
Kintara Therapeutics, Inc.
(Exact name of registrant as specified in its charter)
|
Nevada |
|
99-0360497 |
|
(State or other jurisdiction of incorporation or organization) |
|
(I.R.S. Employer Identification No.) |
12707 High Bluff Dr., Suite 200
San Diego, CA, 92130
(Address of principal executive offices) (Zip Code)
(858) 350-4364
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class |
|
Trading Symbol(s) |
|
Name of each exchange on which registered |
|
Common Stock |
|
KTRA |
|
The Nasdaq Capital Market |
Securities registered pursuant to Section 12(g) of the Act: None.
Indicate by check mark if the registrant is a well-known seasoned issuer as defined in Rule 405 of the Securities Act. ☐ Yes ☒ No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. ☐ Yes ☒ No
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. ☒ Yes ☐ No
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). ☒ Yes ☐ No
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer”, “accelerated filer”, “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
|
☐ |
|
Accelerated filer |
☐ |
|
Non-accelerated filer |
|
☒ |
|
Smaller reporting company |
☒ |
|
Emerging growth company |
|
☐ |
|
|
|
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant is a shell company (as defined by Rule 12b-2 of the Act) ☐ Yes ☒ No
As of December 31, 2019, the aggregate market value of the issued and outstanding common stock held by non-affiliates of the registrant, based upon the closing price of our common stock of $0.6897 was approximately $7.7 million. For purposes of the above statement only, all directors, executive officers and 10% shareholders are assumed to be affiliates. This determination of affiliate status is not necessarily a conclusive determination for any other purpose.
Number of shares of common stock outstanding as of September 15, 2020 was 23,543,892.
DOCUMENTS INCORPORATED BY REFERENCE – None
FOR THE FISCAL YEAR ENDED JUNE 30, 2020
TABLE OF CONTENTS
i
Background
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.) is a clinical stage, biopharmaceutical company focused on the development and commercialization of new cancer therapies.
On June 10, 2020, we entered into an Agreement and Plan of Merger and Reorganization (the “Merger Agreement”), dated as of June 9, 2020, by and among Adgero Acquisition Corp., our wholly-owned subsidiary incorporated in the State of Delaware (“Merger Sub”), and Adgero Biopharmaceuticals Holdings, Inc., a Delaware corporation (“Adgero”). On August 19, 2020, upon the terms and subject to the conditions set forth in the Merger Agreement, Merger Sub merged with and into Adgero (the “Merger”), the separate corporate existence of Merger Sub ceased and Adgero continued its existence under Delaware law as the surviving corporation in the Merger and became our direct, wholly-owned subsidiary. As a result of the Merger, each issued and outstanding share of Adgero common stock, par value $0.0001 per share (the “Adgero Common Stock”) (other than treasury shares held by Adgero), was converted automatically into the right to receive 1.5740 shares (the “Exchange Ratio”) of our common stock, and cash in lieu of any fractional shares. Also, each outstanding warrant to purchase Adgero Common Stock was converted into a warrant exercisable for that number of shares of our common stock equal to the product of (x) the aggregate number of shares of Adgero Common Stock for which such warrant was exercisable and (y) the Exchange Ratio.
Following the completion of the Merger, we changed our name from DelMar Pharmaceuticals, Inc. to Kintara Therapeutics, Inc. and began trading on Nasdaq under the symbol “KTRA”. Unless the context provides otherwise, the “Company,” “we,” “us,” or “our” refers to Kintara and its consolidated subsidiaries, including Adgero.
We are dedicated to the development of novel cancer therapies for patients with unmet medical needs. Our mission is to benefit patients by developing and commercializing anti-cancer therapies for patients whose solid tumors exhibit features that make them resistant to, or unlikely to respond to, currently available therapies, with particular focus on orphan cancer indications.
Our two lead candidates are VAL-083, a novel, validated, DNA-targeting agent, for the treatment of drug-resistant solid tumors such as glioblastoma multiforme (“GBM”) and potentially other solid tumors, including ovarian cancer, non-small cell lung cancer (“NSCLC”), and diffuse intrinsic pontine glioma (“DIPG”) and REM-001, a late-stage photodynamic therapy (“PDT”) for the treatment of cutaneous metastatic breast cancer (“CMBC”). PDT is a treatment that uses light sensitive compounds, or photosensitizers, that, when exposed to specific wavelengths of light, act as a catalyst to produce a form of oxygen that induces local tumor cell death.
Recent Highlights
|
|
• |
On August 21, 2020, we announced we had regained compliance with the minimum bid price requirement for continued listing on The Nasdaq Capital Market. As a result of our shares having had a closing bid price at, or above, $1.00 per share for a minimum of ten (10) consecutive business days, our stock had regained compliance with the minimum bid price requirement and the matter is now closed. |
|
|
• |
On August 19, 2020, we completed our merger with Adgero and through three closings of a private placement, the first of which also closed on August 19, 2020, we raised aggregate gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million. |
|
|
• |
On July 17, 2020, we received a notification of award of a Small Business Technology Transfer grant to study the use of REM-001 in the prevention of arteriovenous fistula maturation failure (“AFMF”), a cardiovascular-related condition that occurs in hemodialysis patients. We believe REM-001 therapy holds promise for certain cardiovascular conditions. This grant will allow us to study the use of REM-001 in the prevention of AFMF further in preclinical models. |
|
|
• |
On June 24, 2020, we announced that we had entered into a $500,000 loan agreement with the National Brain Tumor Society and the National Foundation for Cancer Research to support VAL-083’s preparation for participation in the GBM Adaptive Global Innovative Learning Environment (“GBM AGILE”) study. Actual proceeds were received in July 2020. |
2
|
|
• |
On June 22, 2020, we announced positive interim data from our ongoing two Phase 2 studies of VAL-083 for the treatment of GBM demonstrating improved outcomes over current standard of care as both a first-line treatment and for recurrent GBM. The data, presented in two posters at the 2020 American Association for Cancer Research (“AACR”) Virtual Annual Meeting II, support our planned participation in the GBM AGILE study. We also updated enrollment data in both GBM study arms being conducted at MD Anderson Cancer Center (“MDACC”) in Houston, Texas. |
|
|
• |
On June 4, 2020, we announced the acceptance of an invitation from the Global Coalition for Adaptive Research (“GCAR”) to include VAL-083 in GCAR’s GBM AGILE study, an adaptive clinical study platform in GBM. We expect to utilize the GBM AGILE study to serve as the basis for VAL-083’s new drug application submission and registration. |
Private Placement of Series C Preferred Stock
In conjunction with the closing of the Merger, and through a series of three private placement closings, we issued a total of 25,028 shares of Series C Convertible Preferred Stock (the “Series C Stock”) at a purchase price of $1,000 per share for total aggregate gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million. Each closing of the private placement was priced at-the-market under the rules of the Nasdaq Stock Market.
The Series C Stock was issued in three series (C-1, C-2, and C-3) at conversion prices equal to $1.16, $1.214 and $1.15, respectively. As result, we issued a total of 25,028 shares of Series C Stock, which will be convertible into an aggregate of 21,516,484 shares of common stock. The Series C Stock will be entitled to receive dividends, payable in shares of common stock at a rate of 10%, 15%, 20% and 25% of the number of shares of common stock issuable upon conversion of the Series C Stock, on the 12th, 24th, 36th and 48th month, anniversary of the initial closing of the private placement which occurred on August 19, 2020; provided, that the holder of such shares has not converted the shares of Series C Stock prior to the applicable dividend rate.
In connection with the private placement, we entered into a Placement Agency Agreement (the “Placement Agency Agreement”), with Aegis Capital Corp., which acted as our exclusive placement agent (the “Placement Agent”) for the private placement. Pursuant to the terms of the Placement Agency Agreement, in connection with the three closings of the private placement, we paid the Placement Agent an aggregate cash fee of $2,502,800, a non-accountable expense allowance of $650,840 and issued to the Placement Agent, or its designees, warrants to purchase 2,504 shares of Series C Stock (the “Placement Agent Warrants”). The Placement Agent Warrants have an exercise price of $1,000 per share, provide for a cashless exercise feature and are exercisable for a period of four years from the date of the initial closing of the private placement. The Series C Stock issuable upon exercise of the Placement Agent Warrants will be convertible into shares of common stock and will be entitled to the same dividend rights as the outstanding Series C Stock. In addition, and as compensation for advisory services rendered in connection with the Merger, we issued 571,951 shares of common stock to the Placement Agent.
Targeted Clinical Milestones
(calendar quarters)
Below are our planned, or expected, milestones for the respective time periods noted:
Q4 2020
|
|
• |
VAL-083: First Patient Enrolled - GCAR GBM AGILE Registration Study |
|
|
• |
VAL-083: Top Line Results - Phase 2 Newly-Diagnosed GBM Study |
Q1 2021
|
|
• |
VAL-083: Top Line Results - Phase 2 Recurrent GBM Study |
Q2 2021
|
|
• |
VAL-083: Top Line Results - Phase 2 Adjuvant GBM Study |
|
|
• |
REM-001: First patient enrolled – CMBC lead-in study |
Q4 2021
|
|
• |
REM-001: Top Line Results – CMBC lead-in study |
3
H1 2022
|
|
• |
VAL-083: Graduation from Stage 1 to Stage 2 - GCAR GBM AGILE Registration Study |
Product Pipeline
VAL-083
Background
VAL-083 is a first-in-class, small-molecule, DNA-targeting chemotherapeutic that has demonstrated activity against a range of tumor types in prior Phase 1 and Phase 2 clinical studies sponsored by the US National Cancer Institute (“NCI”). As part of our business strategy, we leverage and build upon these prior NCI investments and data from more than 40 NCI- Phase 1 and Phase 2 clinical studies, which includes an estimated 1,100 patient safety database. We assess the NCI results and our own research to identify and target unmet medical needs in modern cancer care. DNA-targeting agents are among the most successful and widely used treatments for cancer. Their efficacy is based on the ability to bind with a cancer cell’s DNA and interfere with the process of protein production required for growth and survival of cancer cells. “First-in-class” means that VAL-083 embodies a unique molecular structure which is not an analogue or derivative of any approved product, or product under development, for the treatment of cancer.
Prior studies of VAL-083 have shown increased median overall survival benefits versus radiation alone validating the tumor affecting properties of VAL-083. Our recent research has highlighted the opportunities afforded by VAL-083’s unique mechanism of action and its potential to address unmet medical needs in a well-defined and acknowledged biomarker selected population within the larger GBM population. We are thus focusing our initial development efforts on patients whose tumors exhibit biological features that make them resistant to, or unlikely to respond to, currently available therapies as identified by the National Comprehensive Cancer Network (“NCCN”). For example, our research demonstrating VAL-083’s activity in GBM independent of the O6-methyl guanine methyltransferase (“MGMT”) methylation status allows us to focus patient selection based on this important biomarker and thus improve the probability of success in our current and future clinical studies.
4
We are currently conducting two open-label, biomarker driven Phase 2 studies in MGMT-unmethylated GBM. MGMT is a DNA-repair enzyme that is associated with resistance to temozolomide (“TMZ”), the current standard-of-care chemotherapy used in the treatment of GBM. Greater than 60% of GBM patients have MGMT-unmethylated tumors and exhibit a high expression of MGMT, which is correlated with TMZ treatment failure and poor patient outcomes as indicated in the NCCN guidelines for GBM treatment published in September 2017. Our research to-date demonstrates that VAL-083’s anti-tumor activity is independent of MGMT expression. In our current Phase 2 studies we are using MGMT as a biomarker to identify patients for treatment with VAL-083 in three distinct GBM patient populations:
|
|
• |
MGMT-unmethylated GBM, currently comprising two ongoing, separate Phase 2 clinical studies for: |
|
|
• |
GBM patients in two study arms at MD Anderson Cancer Center: |
|
|
• |
as adjuvant therapy immediately following concomitant TMZ treatment with chemoradiation; and |
|
|
• |
in Avastin®-naïve recurrent GBM patients; |
|
|
• |
Newly diagnosed GBM patients at Sun Yat-sen University Cancer Center (“SYSUCC”). |
On June 4, 2020, we accepted an invitation from the Global Coalition for Adaptive Research (“GCAR”) to include VAL-083 in GCAR’s Glioblastoma Adaptive Global Innovative Learning Environment (“GBM AGILE”) Study, an adaptive clinical study platform for patients with GBM. We plan to utilize the GBM AGILE study to serve as the basis for VAL-083’s new drug application submission and registration.
GBM AGILE is an international effort to develop potential therapies for newly-diagnosed and recurrent GBM utilizing an FDA approved master protocol with multiple drugs from multiple sponsors tested simultaneously and over time against a common control arm with a primary endpoint of overall survival. We intend to use results from the VAL-083 arm of the GBM AGILE study to file for FDA approval, assuming results support such a filing. GBM AGILE is a Phase II/Phase III study which employs a cost-efficient, adaptive study design with a Stage 1 learning and adapting phase and a Stage 2 expansion and confirmation phase. GBM AGILE will consist of up to a maximum 200 patients stratified by three subtypes: newly-diagnosed methylated, newly-diagnosed unmethylated, and recurrent. The effort is led by key opinion leaders in the GBM field and has the collective support of an international group of more than 130 clinicians, researchers, biostatisticians, imagers, pathologists, leaders from government and industry, and patient advocates.
GCAR is a 501(c)(3) organization that functions as GBM AGILE study sponsor, and provides financial support for the program infrastructure, as well as general study oversight. Comprising leading clinical, translational, and basic science investigators, GCAR strives to support the development of novel treatments to fight against rare and deadly diseases like GBM where patient prognosis is poor and treatment options are limited. Other key strategic partners for the GBM AGILE study effort include the National Brain Tumor Society, National Foundation for Cancer Research, and Asian Fund for Cancer Research. These nonprofit organizations are working together to provide philanthropic support as well as assistance in communicating with patients and families and inviting all others to join in supporting this innovative approach to brain tumor treatment development.
We have also undertaken research in ovarian cancer. Ovarian cancer is the fifth most common cancer in women and is the leading cause of death among women diagnosed with gynecological malignancies. We are in the process of evaluating the best path forward in ovarian cancer including the potential combination of VAL-083 with PARP inhibitors. The FDA granted orphan drug designation for the use of VAL-083 in the treatment of ovarian cancer in 2016.
In addition to our clinical development activities in the United States, pursuant to our collaboration with Guangxi Wuzhou Pharmaceutical (Group) Co. Ltd. (“Guangxi Wuzhou Pharmaceutical Company”), we have provided Guangxi Wuzhou Pharmaceutical Company certain commercial rights to VAL-083 in China where it is approved as a chemotherapy for the treatment of chronic myelogenous leukemia (“CML”) and lung cancer. Guangxi Wuzhou Pharmaceutical Company is the only manufacturer presently licensed by the China Food and Drug Administration (“CFDA”) to produce the product for the China market.
We have a broad patent portfolio to protect our intellectual property. Our patent applications claim composition of matter and methods of use of VAL-083 and related compounds, synthetic methods, and quality controls for the manufacturing process of VAL-083. We believe that our portfolio of intellectual property rights provides a defensible market position for the commercialization of VAL-083. In addition, VAL-083 has been designated by the FDA as an orphan drug under the Orphan Drug Act and the European Medicines Agency (“EMA”) for the treatment of gliomas, including GBM. The FDA has also granted Orphan Drug description to VAL-083 for the treatment of medulloblastoma and ovarian cancer.
5
Our corporate development strategy is to advance VAL-083 on an indication-by-indication basis, and then to consider out-licensing when it has matured enough to warrant proper licensing valuations. In addition to VAL-083’s applicability to multiple solid tumor indications, we are also constantly evaluating licensing, or acquiring additional product candidates, in order to establish a product pipeline and to position us for long-term sustainability and growth of shareholder value. We believe the experience of our clinical development team will position us to efficiently develop possible drug candidates that we may acquire, or license, in the future.
We intend to continue to evaluate options for our strategic direction. These options may include raising additional capital, the acquisition of another company and/or complementary assets, our sale, or another type of strategic partnership.
MGMT-unmethylated GBM
GBM is the most common and the most lethal form of glioma. According to the Central Brain Tumor Registry of the United States, GBM occurs with an incidence of 3.20 per 100,000 person-years. Approximately 13,000 new cases of GBM were diagnosed in the United States and 16,000 in Europe during 2017. Within the GBM patient population, approximately two-thirds of patients are unmethylated with respect to their MGMT status.
Measurement of MGMT (O6-methyl guanine methyltransferase) methylation status has become routine in clinical practice as a biomarker that correlates with resistance to the standard-of-care chemotherapy with TMZ (Temodar®), and patient outcomes in GBM. Approximately two-thirds of GBM patients’ tumors are characterized as “MGMT-unmethylated” and exhibit a high expression of MGMT, a naturally occurring DNA-repair enzyme, the activity of which nullifies the chemotherapeutic activity of TMZ. The lack of specific therapies for MGMT-unmethylated GBM is a significant unmet medical need. Importantly, the 2017 update to the NCCN guidelines states that the treatment benefit of TMZ is likely to be lower in GBM patients with an unmethylated MGMT promoter.
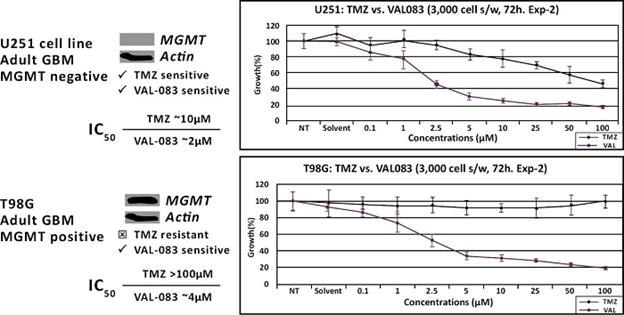
We have demonstrated that VAL-083’s anti-tumor mechanism is active independent from the MGMT status in vitro. We believe this suggests the potential of VAL-083 as a replacement for the current standard-of-care chemotherapy, temozolomide, in MGMT-unmethylated GBM. We are therefore utilizing MGMT-methylation status to identify GBM patients who are unlikely to respond to temozolomide and including only MGMT-unmethylated patients in our current clinical studies of VAL-083.
We believe that our research, in the context of the 2017 update to the NCCN guidelines, highlights this unmet need and the opportunity for VAL-083 as a potential new standard-of-care in the treatment of MGMT-unmethylated GBM.
VAL-083 Clinical Studies
Phase 2 Study in Newly-Diagnosed MGMT-unmethylated GBM
In September 2017, we initiated a single arm, biomarker driven, open-label Phase 2 study in newly-diagnosed MGMT-unmethylated GBM patients at SYSUCC in Guangzhou, China. The study is being conducted under our collaboration agreement with Guangxi Wuzhou Pharmaceutical Company.
In this Phase 2 study, VAL-083 is being combined with radiotherapy as a potential replacement for standard-of-care chemoradiation with temozolomide in patients with MGMT-unmethylated GBM. The goals of the study are to confirm the safety of the three-day VAL-083 dosing regimen in combination with radiotherapy and to investigate efficacy outcomes of the combination of VAL-083 and radiotherapy in MGMT-unmethylated GBM patients.
We have completed enrollment of this study with a total of 29 newly-diagnosed, MGMT-unmethylated GBM patients. The efficacy endpoints of the study include tumor response, as assessed by the Response Assessment in NeuroOncology (“RANO”), and progression-free survival (“PFS”), progression-free survival at six months (“PFS6”), and overall survival (“OS”), compared to historical results in the target population. The study is being conducted in two parts: (1) Dose-confirmation: VAL-083 in cohorts (20, 30 and 40 mg/m2/day IV daily x 3 every 21 days) to assess safety and activity when administered concurrently with x-ray therapy (“XRT”) to confirm the maximum tolerated dose (“MTD”), and (2) Expansion: VAL-083 will be studied in up to 20 additional patients at the target dose, as determined by the dose-confirmation part of the study, administered concurrently with XRT. Assessments of safety and tolerability will be used to support further clinical development of VAL-083 in combination with radiotherapy. Pharmacokinetic assessments of VAL-083 in plasma and cerebral spinal fluid (“CSF”) will be used to correlate drug exposure in the central nervous system with patient outcomes.
Dose-confirming cohorts studying 20, 30, and 40 mg/m2/day x three every 21 days have been completed. Based on the dose confirmation phase of the study, we have selected 30 mg/m2/day for combination with irradiation for the treatment of newly-diagnosed MGMT-unmethylated GBM patients. This study is fully enrolled at 29 patients.
6
On June 22, 2020 at the AACR’s Virtual Annual Meeting II, we provided an update on patient data as follows:
|
|
• |
For the 25 patients initially receiving the treatment dose that will be carried forward in the GBM AGILE pivotal study (30 mg/m2/day on days 1, 2 and 3 of a 21-day cycle) median progression-free survival (“PFS”) was reported to be 8.7 months (confidence interval, or CI 6.0-12.0 months) as of the May 15, 2020 cut-off date. |
|
|
• |
Overall PFS (n=29) with VAL-083 was also 8.7 months (CI 6.4-11.2 months). |
While this is not a head-to-head study, historically, temozolomide (“TMZ”) has been demonstrated to have 6.9 months PFS in unmethylated GBM patients. Other doses were also examined as part of the dose escalation aspect of the study, and all but the 20 mg/m2/day dose also demonstrated superior PFS to the historical comparator. A median of eight cycles of treatment has been received by all patients who had either completed treatment, or remain in active treatment. Nine patients have received ten or more cycles.
Through our research, and that of the NCI, we have previously demonstrated that VAL-083 crosses the blood brain barrier. Preliminary data from the SYSUCC study indicate that the concentration of VAL-083 is generally as high in CSF as in plasma at two hours post-infusion.
Concentration of VAL-083 — Two Hours Post Dose
|
|
|
|
|
|
|
Mean Concentrations (ng/mL) |
|
|
|
|
|
|||||
|
Dose (mg/m2) |
|
n |
|
|
Plasma (2 hours post dose) |
|
|
CSF (2 hours post dose) |
|
|
Conc. Ratio @ 2 hours CSF/Plasma |
|
||||
|
20 |
|
|
1 |
|
|
|
110 |
|
|
|
154 |
|
|
|
1.40 |
|
|
30 |
|
|
3 |
|
|
|
97 |
|
|
|
134 |
|
|
|
1.41 |
|
|
40 |
|
|
3 |
|
|
|
170 |
|
|
|
190 |
|
|
|
1.13 |
|
By comparison, temozolomide is typically 80% lower in the CSF than the plasma (Schreck et al. 2018, Oncology (Williston Park)). The accumulation of VAL-083 in the CSF further validates that VAL-083 crosses the blood-brain-barrier and demonstrates that therapeutic drug concentrations in the CSF are achievable for extended periods of time.
Phase 2 Study in MGMT-unmethylated GBM in Collaboration with University of Texas MD Anderson Cancer Center
In February 2017, we initiated a biomarker driven, open-label, single-arm Phase 2 study in collaboration with MDACC. This biomarker-driven study (testing for MGMT methylation status) has been amended to enroll up to 83 patients (35 with a starting dose of 40 mg/m2/day and 48 with a starting dose of 30 mg/m2/day) to determine the potential of VAL-083 treatment to improve overall survival in GBM patients whose tumors have recurred following treatment with temozolomide. These patients will not have been treated previously with Avastin®. In addition, this study has been amended to add a new adjuvant patient arm. This arm will include up to 36 patients previously treated with TMZ in combination with radiation who, rather than being treated with additional cycles of TMZ, will begin treatment with VAL-083.
Recurrent Study Arm
The patients in the recurrent study arm are receiving second-line therapy with VAL-083 following TMZ failure. As of May 28, 2020, 72 patients (out of a planned 83) have been enrolled in the recurrent arm of this study.
On June 22, 2020 at the AACR’s Virtual Annual Meeting II, we provided an update on patient data as follows:
|
|
• |
In recurrent GBM, for the 37 patients initially receiving the intended treatment dose that will be carried forward in the GBM AGILE pivotal study (30 mg/m2/day on days 1, 2 and 3 of a 21-day cycle), median overall survival (mOS) is currently 8.5 months (CI 5.7-14.3 months) as of the May 28, 2020 cut-off date. |
|
|
• |
Overall mOS for the 72 patients who have completed at least one cycle of treatment was 7.1 months (CI 5.8-9.9 months). |
The safety profile in this study has been well within the existing safety monitoring guidelines described in the study protocol. However, in consultation with the principal investigator at MDACC, we have amended the protocol for this clinical study to modify the starting dose of VAL-083 to 30 mg/m2/day on days 1, 2 and 3, of a 21-day cycle. This modification may improve tolerance in this patient population and thereby potentially increase overall exposure to VAL-083 by increasing the number of cycles of drug patients may be able to receive. We have modified the patient screening platelet count, from 100,000/µL to 125,000/µL, for the same reasons. Safety data from this study will become part of the overall safety dossier to support future filings with the FDA and other regulatory agencies.
7
It is important for this GBM patient population, which has been heavily pre-treated with temozolomide, to be able to be treated with multiple cycles of VAL-083 without significant hematological toxicities. We believe the modified dose of VAL-083, in addition to the change in patient eligibility platelet counts, should help provide for enhanced patient safety. We believe a positive outcome from this study will help support approval of VAL-083 for the treatment of MGMT-unmethylated recurrent GBM.
A detailed description of this study can be found at clinicatrials.gov, Identifier Number: NCT02717962.
Adjuvant Study Arm
On July 24, 2019, we announced the enrollment of the first patient in the adjuvant arm of the Phase 2 study being conducted at MDACC. The adjuvant arm was originally planned for 24 patients, but based on encouraging outcomes, we plan to increase the adjuvant arm enrollment from the originally planned 24 patients to include up to 12 additional patients. These patients will have had initial cycles of temozolomide concomitant with radiation but will not have yet started subsequent cycles of TMZ (i.e., maintenance stage TMZ patients). Published data from Tanguturi et al (2017 Nero-Oncology) indicates that MGMT-unmethylated patients receiving current standard of care have a median progression-free survival of 6.9 months.
On June 22, 2020 at the AACR’s Virtual Annual Meeting II, we provided an update on patient data as follows:
|
|
• |
As of the data cut-off date of May 28, 2020, 19 evaluable subjects have completed at least one 21-day cycle of treatment, with a total of 25 subjects enrolled. Enrollment for this arm was initiated in July 2019, and all 25 subjects enrolled to-date were alive at the data cut-off date. |
As noted above, patients in the recurrent arm of the MDACC clinical study have been heavily pre-treated with temozolomide. Based on published data from our MDACC and SYSUCC clinical studies, we believe there is a significant opportunity to treat GBM patients in the pre-temozolomide maintenance stage (i.e., adjuvant). At the AACR’s annual meeting in April 2019, we reported that myelosuppression (thrombocytopenia and neutropenia) is the most common adverse event associated with VAL-083.
Safety Across Studies
Three subjects have experienced a serious adverse event (“SAE”), possibly related to VAL-083 in the newly-diagnosed study as of May 15, 2020, while as of May 28, 2020, 10 subjects have experienced a possibly drug-related SAE in the recurrent arm of the Phase 2 Study in MGMT-unmethylated GBM, and one patient has experienced a possibly drug-related SAE in the adjuvant arm of that study.
VAL-083 Fast Track Designation
The FDA has granted us Fast Track designation for VAL-083 in recurrent GBM.
Fast Track designation is designed to expedite the review of drugs that show promise in treating life-threatening diseases and address unmet medical needs, with the goal of getting new treatments to patients earlier. Fast Track designation provides sponsors with an opportunity for increased frequency for communication with the FDA to ensure an optimal development plan and to collect appropriate data needed to support drug approval. Additional benefits of the Fast Track designation may include an Accelerated Approval, a Priority Review, and a Rolling Review. Accelerated Approval is granted to drugs that demonstrate an effect on a surrogate, or intermediate endpoints, reasonably likely to predict clinical benefit. Priority Review shortens the FDA review process for a new drug from ten months to six months and is appropriate for drugs that demonstrate significant improvements in both safety and efficacy of an existing therapy. Rolling Review provides a drug company the opportunity to submit completed sections of its New Drug Application (“NDA”) for review by the FDA. Typically, NDA reviews do not commence until the drug company has submitted the entire application to the FDA. Through the Fast Track designation, the FDA attempts to ensure that questions raised during the drug development process are resolved quickly, often leading to earlier approval and increased access for patients.
Current Treatments for Gliomas and Glioblastoma Multiforme
Gliomas are a type of Central Nervous System (“CNS”) tumor that arises from glial cells in the brain or spine. Glial cells are the cells surrounding nerves. Their primary function is to provide support and protection for neurons in the CNS.
GBM is the most common and the most lethal form of glioma. According to the Central Brain Tumor Registry of the United States, GBM occurs with an incidence of 3.20 per 100,000 person-years. Approximately 13,000 new cases of GBM were diagnosed in the United States and 16,000 in Europe during 2017.
8
Common symptoms of GBM include headaches, seizures, nausea, weakness, paralysis and personality or cognitive changes such as loss of speech or difficulty in thinking clearly. GBM progresses quickly and patients’ conditions deteriorate rapidly progressing to death. The outlook for GBM patients is generally poor. The overall median survival in newly diagnosed GBM patients with best available treatments is less than 15 months, and two-year and five-year survival rates are approximately 30% and 10%, respectively. Median overall survival in newly-diagnosed, unmethylated GBM patients is 12.2 months.
In September 2017, the NCCN updated treatment guidelines for GBM. The recommended treatment regimen for GBM includes surgical resection to remove as much of the tumor as possible (“debulking”) followed by radiotherapy with concomitant and adjuvant chemotherapy with temozolomide with or without tumor treating fields (“TTF”). GBM patients whose tumors exhibit an unmethylated promoter for the gene encoding the DNA repair enzyme MGMT, a biomarker correlated with resistance to temozolomide, may be treated with radiation alone following surgery.
Patients with an unmethylated MGMT promoter have high levels of MGMT, a naturally-occurring DNA repair enzyme that repairs tumor-fighting lesions induced by TMZ thus allowing a patient’s tumor to continue to grow despite treatment, which leads to poor outcomes. Measurement of MGMT methylation status has become routine in clinical practice as biomarker that correlates with response to TMZ and patient outcomes in GBM.
Probability of GBM Patient Survival Correlated to Expression of MGMT Enzyme (Unmethylated promoter = High MGMT Expression and Significantly Shorter Survival)

TTF (Optune®) is a non-invasive technique for adults with GBM. TTF uses alternating electrical fields to disrupt tumor cell division, or cause cell death, thereby preventing the tumor from growing or spreading as quickly. A clinical study reported that GBM patients treated with TTF combined with TMZ experienced longer survival than those treated with TMZ alone.
The majority of GBM patients’ tumors recur within 6 – 12 months of initial treatment. Experimental therapy through clinical studies is recommended under NCCN guidelines for eligible patients. NCCN guidelines also recommend treatment with systemic chemotherapy, such as lomustine (“CCNU”). For patients who are eligible for additional surgical debulking, local chemotherapy with carmustine (“BCNU”) wafers may be employed. CCNU and BCNU target the same DNA-site as TMZ and are also subject to MGMT-related resistance.
Avastin (Avastin®, an anti-VEGF antibody) recently received full approval in the US, Canada, Australia, and Japan as a single agent for patients with recurrent GBM following prior therapy. Avastin carries an FDA “black-box warning” related to severe, sometimes fatal, side effects such as gastrointestinal perforations, wound healing complications and hemorrhage. There are no data demonstrating an improvement in disease-related symptoms or increased survival for GBM patients treated with Avastin.
Recurrent GBM patients, especially those whose tumors progress following treatment with Avastin, have limited or no treatment options and a very poor prognosis. According to published literature, the median survival for GBM patients whose tumors progress following Avastin is less than five months.
9
VAL-083 Mechanism of Action
Chemotherapy forms the basis of treatment in nearly all cancers. We believe that VAL-083 may be effective in treating tumors exhibiting biological features that cause resistance to currently available chemotherapy, particularly for patients who have failed, or become resistant to, other treatment regimens.
Based on published research and our own data, the cytotoxic functional groups, and the mechanism of action of VAL-083 are functionally different from alkylating agents commonly used in the treatment of cancer. VAL-083 has previously demonstrated activity in cell-lines that are resistant to other types of chemotherapy. No evidence of cross-resistance has been reported in published clinical studies.
Our research suggests that VAL-083 attacks cancer cells via a unique mechanism of action which is distinct from other chemotherapies used in the treatment of cancer. Our data indicate that VAL-083 forms inter-strand crosslinks at the N7 position of guanine on the DNA of cancer cells. Our data also indicate that this crosslink forms rapidly and is not easily repaired by the cancer cell, resulting in cell-cycle arrest and lethal double-strand DNA breaks in cancer cells. VAL-083 readily crosses the blood brain barrier. Published preclinical and clinical research demonstrate that VAL-083 is absorbed more readily in tumor cells than in normal cells.
In vitro, our data also demonstrate that VAL-083’s distinct mechanism may be able to overcome drug resistance against a range of cancers. For example, VAL-083 is active against MGMT-unmethylated GBM cells which are resistant to treatment with temozolomide and nitrosoureas. VAL-083 also retains a high level of activity in p53 mutated non-small cell lung cancer (“NSCLC”), ovarian cancer and medulloblastoma cell lines that are resistant to platinum-based chemotherapy.
Importantly, clinical activity against each of the tumors mentioned above was established in prior NCI-sponsored Phase 2 clinical studies. We believe that these historical clinical data and our own research support the development of VAL-083 as a potential new treatment for multiple types of cancer.
The main dose-limiting toxicity (“DLT”) related to the administration of VAL-083 in previous NCI-sponsored clinical studies and our own clinical studies is myelosuppression, particularly thrombocytopenia. Myelosuppression, including thrombocytopenia, is a common side effect of chemotherapy. Myelosuppression is the decrease in cells responsible for providing immunity, carrying oxygen, and causing normal blood clotting. Thrombocytopenia is a reduction in platelet counts which assist in blood clotting. Modern medicine allows for better management of myelosuppressive side effects. We believe this offers the potential opportunity to improve upon the drug’s already established efficacy profile by substantially increasing the dose of VAL-083 that can be safely administered to cancer patients.
There is no evidence of lung, liver, or kidney toxicity even with prolonged treatment by VAL-083. Data from the Chinese market where the drug has been approved for more than 15 years supports the safety findings of the NCI studies.
10
VAL-083 is Active Independent of MGMT
We have presented data at several peer reviewed meetings demonstrating that VAL-083 is active independent of MGMT resistance in GBM cell lines and other CNS tumor cells. Our research, along with that of others, demonstrates that VAL-083’s unique cytotoxic mechanism forms DNA cross-links at the N 7position of guanine and retains cytotoxic activity independent of MGMT expression in vitro. Our studies demonstrate that VAL-083 has more potent activity against brain tumor cells in comparison to TMZ and overcomes resistance associated with MGMT, suggesting the potential to surpass the current standard-of-care in the treatment of GBM.
In addition, historical NCI clinical study data and our own research support the activity of VAL-083 as a potentiator of radiotherapy. Radiotherapy in combination with temozolomide is the current standard of care in the treatment of newly diagnosed GBM. Our research demonstrates that temozolomide and radiotherapy are ineffective against GBM cells exhibiting a high expression of MGMT, whereas VAL-083 potentiates the tumor-killing effect of radiation independent of MGMT expression. Furthermore, the combination of VAL-083 and radiation has been demonstrated to be active against GBM cancer stem cells (“CSCs”) in vitro. CSCs are often resistant to chemotherapy and form the basis for tumor recurrence and metastasis. GBM CSCs display strong resistance to TMZ, even where MGMT expression is low. However, our data demonstrates that GBM CSCs are susceptible to VAL-083 independent of MGMT expression.
Other Indications for VAL-083—Potential Future Opportunities
VAL-083 in Ovarian Cancer
With the US Food and Drug Administration (“FDA”) approval for our investigational new drug application (“IND”) for ovarian cancer, we have future plans for a phase 1/2, open-label, multicenter study of VAL-083 in patients with Recurrent Platinum Resistant Ovarian Cancer (“REPROVe”). Platinum-based chemotherapy is the standard-of-care in the treatment of ovarian cancer. Nearly all ovarian cancer patients eventually become resistant to platinum (“Pt”) based chemotherapy leading to treatment failure and poor patient outcomes. We have demonstrated that VAL-083 is active against Pt-resistant ovarian cancer in vitro. However, based on ongoing evaluation and input from our ovarian cancer advisory board, we are reassessing the development of VAL-083 for the treatment of ovarian cancer. We are in the process of evaluating the best path forward in ovarian cancer and are evaluating strategic options, including the potential combination of VAL-083 with PARP inhibitors. As a result, we have inactivated the IND while we explore alternative study designs.
VAL-083 in Lung Cancer
Lung cancer is a leading cause of cancer death around the world and effective treatment for lung cancer remains a significant global unmet need despite advances in therapy. Incidence of lung cancer in the United States is approximately 47 per 100,000 with the majority (85%) being NSCLC, the most common type of lung cancer. Globally, the market for lung cancer treatment may exceed $24 billion by 2033 according to a report published by Evaluate Pharma.
11
The activity of VAL-083 against solid tumors, including lung cancer, has been established in both preclinical and human clinical studies conducted by the NCI. We have developed nonclinical data to support the utility of VAL-083 in the modern treatment of lung cancer. In an established murine xenograft model of NSCLC, the activity of VAL-083 was compared to standard platinum-based therapy with cisplatin against human NSCLC cell lines A549 (TKI-sensitive) and H1975 (TKI-resistant). In the study, VAL-083 demonstrated superior efficacy and safety in the treatment of TKI-susceptible (A549) tumors and in TKI-resistant (H1975) tumors.
Central Nervous System Metastases of Solid Tumors
The successful management of systemic tumors by modern targeted therapies has led to increased incidence of mortality due to CNS metastases of lung cancer and other solid tumors. In June 2013, we split our Phase 1/2 clinical study protocol into two separate studies: one focusing solely on refractory GBM and the other focusing on secondary brain cancers caused by other tumors that have spread to the brain.
Based on historical clinical activity and our own research, we believe that VAL-083 may be suitable for the treatment of patients with CNS metastases who currently have limited treatment options. Subject to the availability of financial and operating resources, we plan to develop a separate protocol for the continued exploration of VAL-083 in patients with secondary brain cancer caused by a solid tumor spreading to the brain.
Pediatric Brain Tumors
Tumors of the brain and spine make up approximately 20 percent of all childhood cancers and they are the second most common form of childhood cancer after leukemia.
The activity of VAL-083 against childhood and adolescent brain tumors has been established in both preclinical and human clinical studies conducted by the NCI. We have presented data indicating that VAL-083 offers potential therapeutic alternatives for the treatment of pediatric brain tumors including SHH-p53 mutated medulloblastoma. In March 2016, the FDA granted orphan drug designation for the use of VAL-083 in the treatment of medulloblastoma. Subject to the availability of resources, we intend to collaborate with leading academic researchers for the continued exploration of VAL-083 as a potential treatment of childhood brain tumors.
Additional Indications for VAL-083
In historical studies sponsored by the NCI in the United States, VAL-083 exhibited clinical activity against a range of tumor types including central nervous system tumors, solid tumors, and hematologic malignancies. We have gathered nonclinical data supporting the activity of VAL-083 in different types of cancer that are resistant to modern targeted therapies and we believe that the unique cytotoxic mechanism of VAL-083 may provide benefit to patients in a range of indications. We intend to continue to research these opportunities, and if appropriate, expand our clinical development efforts to include additional indications.
VAL-083 Target Markets
|
VAL-083 target markets |
|
2024 Estimated Global Sales |
|
Glioblastoma multiforme (GBM) |
|
$1.5B |
|
Ovarian Cancer |
|
$4.2B |
|
Non-small cell lung cancer (NSCLC) |
|
$32.6B |
Source: Evaluate Pharma
DNA-targeting agents such as alkylating agents or platinum-based chemotherapy form the mainstay of chemotherapy treatments used in the treatment of cancers. For example, TMZ had peak annual sales of $1.1 billion in 2010, while bendamustine, had peak annual sales of $0.8 billion in 2014.
We believe VAL-083 is a first-in-class DNA targeting agent with a novel mechanism of action. VAL-083’s anti-cancer activity was established in a range of tumor types in prior NCI-sponsored clinical studies. Based on this novel mechanism, we have demonstrated that the anti-cancer activity is maintained against tumor cells that are resistant to other DNA-targeting agents. We believe this positions VAL-083 as a potential chemotherapy-of-choice for patients whose tumors are resistant to current standard-of-care chemotherapy in orphan and major cancer indications.
12
Our ongoing research and development activities are focused on indications where VAL-083 demonstrated promising activity in prior NCI-sponsored studies and where our research suggests an opportunity to address significant unmet medical needs due to the failure of existing treatments.
Glioblastoma Multiforme
GBM is the most common and the most lethal form of glioma. According to the Central Brain Tumor Registry of The United States, GBM occurs with an incidence of 3.20 per 100,000 person-years. Approximately 13,000 new cases of GBM were diagnosed in the United States and 16,000 in Europe during 2017.
Newly diagnosed patients suffering from GBM are initially treated through invasive brain surgery, although disease progression following surgical resection is nearly 100%. Temozolomide (Temodar®) in combination with radiation is the front-line therapy for GBM following surgery. Global revenues of branded Temodar reached $1.1 billion in 2010. Approximately 60% of GBM patients treated with Temodar® experience tumor progression within one year. Median overall survival in newly-diagnosed, unmethylated GBM patients is 12.2 months.
Bevacizumab (Avastin®) has been approved for the treatment of GBM in patients failing Temodar®. In clinical studies, approximately 20% of patients failing Temodar® respond to Avastin® therapy and no improvement in median survival was reported.
The market for refractory (Avastin-failed) GBM is limited to those jurisdictions where Avastin is approved for the treatment of GBM. The United States, Canada, Australia, Japan and Switzerland represent the major markets where Avastin is used in the treatment of GBM.
Based on a November 2018 report from GlobalData, we believe there is a projected market opportunity for GBM of approximately $800 million, estimated to reach approximately $1.8 billion by 2027.
REM-001
Background
Through REM-001, we are developing our photodynamic therapy (“PDT”) for the treatment of rare, unmet medical needs. PDT is a treatment that uses light sensitive compounds, or photosensitizers, that, when exposed to specific wavelengths of light, act as catalysts to produce a form of oxygen that induces local tumor cell death. REM-001 consists of three parts, the laser light source, the light delivery device, and the REM-001 drug product (collectively, the “REM-001 Therapy”). REM-001 consists of an active pharmaceutical ingredient (“API”) in a lipid formulation. The REM-001 API is SnET2 (“tin ethyl etiopurpurin”) which is a second-generation PDT photosensitizer agent. We believe REM-001 possesses multiple advantages over earlier generation PDT compounds. Our lead indication for REM-001 is CMBC which is a disease that may strike individuals with advanced breast cancer and for which effective treatment options are limited. In four Phase 2 and/or Phase 3 clinical atudies in CMBC patients, primarily targeting patients who had previously received chemotherapy and failed radiation therapy, REM-001 Therapy was able to reduce or eliminate a substantial number of the treated CMBC tumors. Specifically, our analysis of the data collected from these studies indicates that in approximately 80% of evaluable tumor sites treated with REM-001 Therapy, there was a complete response; meaning that follow-up clinical assessments indicated no visible evidence of the tumor remaining. We believe clinical data indicates that REM-001 Therapy holds promise as a treatment to locally eliminate, or slow the growth of, treated cutaneous cancerous tumors in this difficult-to-treat patient population.
In 2012, Adgero acquired certain assets and regulatory filings, including REM-001 Therapy developed by Miravant Medical Technologies, and its wholly-owned subsidiaries, a former public pharmaceutical and research development company (collectively, “Miravant”), and the associated technology, clinical data and intellectual property, from a creditor of Miravant. Between February 1996 and January 1999, Miravant, with support from certain corporate partners, conducted four Phase 2 and/or Phase 3 clinical studies for the treatment of CMBC using REM-001 Therapy (collectively, the “Miravant CMBC Studies”). The primary motivation behind our acquisition of the technology was to secure the rights to the REM-001 Therapy and its associated technology, proprietary processes and regulatory filings which have already undergone substantial clinical development which we believe will help expedite the process of gaining regulatory approval to market our REM-001 Therapy.
Miravant initiated commercial development of REM-001 and its associated device components in the 1990s. This led to late-stage clinical studies in CMBC and also in an aspect of “wet” age-related macular degeneration (“AMD”) a disease that affects over 1.5 million people in the United States and is a cause of vision loss in older individuals. Of these two indications, AMD represented a much larger market, and in 1998, for what we believe were primarily business reasons, Miravant discontinued its CMBC program and, together with, or through its corporate partners, ultimately focused its REM-001 development efforts on AMD. In 2004, Miravant
13
submitted a new drug application (“NDA”) to the FDA for the use of REM-001 to treat an aspect of AMD. The FDA reviewed this submission and granted Miravant an approvable letter for REM-001 in the treatment of AMD, with final approval contingent on, among other things, the successful completion of a Phase 3 study. Miravant ceased operations in 2006 prior to completing this study.
While Miravant did not pursue the CMBC indication through to approval, it did compile substantial clinical data in the four Miravant CMBC Studies. The first two of these studies were Phase 2/3 studies that treated 68 CMBC patients who, for the most part, previously failed radiation therapy, and were then treated with REM-001 Therapy. Miravant compiled both safety and efficacy data for these two studies. At the time Miravant discontinued its CMBC program, REM-001 Therapy was also being tested in two additional Phase 2 or 3 clinical studies that treated a total of 81 patients. Our review of internal Miravant records indicates that data was collected in all four studies generally in accordance with Good Clinical Practice and the data was analyzed for safety, and reports were filed with the FDA. Our review also indicates that Miravant never conducted an efficacy analysis of the 81 patients in the last two studies which were not yet complete when Miravant discontinued its CMBC program.
Since acquiring the rights to REM-001 Therapy, we have performed a preliminary analysis of the data collected from the 81 patients that Miravant never analyzed for efficacy. Based on our analysis of both that data, and data collected from the initial 68 patients, we believe REM-001 Therapy provided promising safety and efficacy in CMBC patients and that, taken together, these results provide strong support for REM-001 Therapy as a potential therapy for this disease. Furthermore, we believe the approvable letter previously granted to Miravant with respect to its NDA for REM-001 in an aspect of AMD may indicate that many of the elements required for approval have already been completed for REM-001.
Numerous approaches have been utilized to treat CMBC patients, including various forms of chemotherapy, radiation therapy, surgical excision, hyperthermia, cryotherapy, electro-chemotherapy, topical drugs, and intra-lesional chemotherapy injections. However, for the most part, we believe that these therapies are often inadequate given the limited efficacy, toxicities and/or side effects of each. We believe our REM-001 Therapy has several advantages for this indication: it can be highly directed to the tumor site, has minimal systemic effects or normal tissue toxicities, can be used in conjunction with other therapies, and can be periodically repeated. Our analysis of the data collected from the Miravant CMBC Studies indicates that in approximately 80% of evaluable tumor sites treated with REM-001 Therapy, there was a complete response, meaning that follow-up clinical assessments indicated no visible evidence of the tumor remaining. Based on these results, we believe that REM-001 Therapy also holds promise as a treatment for other cutaneous metastatic cancers and locally advanced basal cell carcinomas.
Our initial product goal is to achieve marketing approval of REM001 Therapy for the treatment of CMBC in the United States. We conducted a preliminary analysis of existing REM001 Therapy clinical study data for CMBC, including data from the Miravant CMBC Studies. We then conducted a more in-depth analysis that was overseen by regulatory experts who have expertise in interacting with the FDA. The consultants we have engaged were either former FDA employees with directly related experience in reviewing similar oncology treatments, or individuals who have provided senior regulatory guidance to major pharmaceutical or medical device companies in situations that led to regulatory approval. The results of this second more in-depth analysis were consistent with our original analysis. As a result of our review, we submitted questions to the FDA under a Type C format to review the technology and results and determine the anticipated requirements for regulatory approval. On March 3, 2017, we received FDA’s written response to these questions. Based on that response, we believe our plans to manufacture REM-001 by revising the prior quality standards to meet the currently-recommended regulatory standards will be acceptable. The FDA also indicated our plans for utilizing light delivery devices that have been shown to be functionally equivalent to the devices used by Miravant will be acceptable.
In October 2017, we held a Type B face-to-face guidance meeting with the FDA that was primarily focused on the design of a Phase 3 study in CMBC. Then, in May 2018, we held a Type B end-of-phase 2 meeting with the FDA that focused on our plans for addressing CMC and device topics related to our CMBC effort. In these interactions, the FDA provided guidance on a number of clinical parameters it would like us to measure in the planned clinical study, and on the associated CMC and device plans. Based on the FDA’s responses, we plan to conduct a Phase 3 clinical study in CMBC to test the safety and efficacy of REM-001 Therapy for marketing approval. In June 2018, we submitted to the FDA a Phase 3 protocol and statistical analysis plan incorporating feedback received from FDA at the October 2017 meeting. We have also undertaken extensive discussions with clinical research organizations to carry out this study and have received detailed proposals from five of these organizations. Since our May 2018 meeting, we have engaged a contract manufacturer who has manufactured the starting material for our API, manufactured two API lots under GMP. We are currently planning to undertake GMP manufacturing of finished drug product for use in the planned clinical study.
We also believe REM-001 Therapy holds promise as a treatment for cutaneous metastatic cancers other than CMBC, as well as locally-advanced basal cell cancer such as often occurs in patients with Basal Cell Carcinoma Nevus Syndrome (“BCCNS”) and cutaneously recurrent basal cell cancer. On January 16, 2018, the FDA granted our request that tin ethyl etiopurpurin (the active pharmaceutical ingredient in REM-001) be designated as an orphan drug for treatment of BCCNS. Following this designation, we contacted clinical experts in BCCNS and related indications to seek their guidance on the most appropriate clinical pathway for REM-001 Therapy in these indications.
14
We believe REM-001 Therapy also holds promise for certain cardiovascular conditions, including prevention and de novo treatment of cardiovascular access sites in hemodialysis patients. We also hold an orphan drug designation that was initially awarded to Miravant for tin ethyl etiopurpurin for the prevention of access graft disease in hemodialysis patients. We have been working to further develop this indication, including engaging with a key opinion leader in this area and submitting an NIH grant proposal for late stage preclinical research that we believe could lead directly to an IND and clinical study. We recently received notification that that grant has been awarded.
REM-001 Regulatory Filings
The initial investigational new drug (“IND”) filing for REM-001 Therapy was IND 39,940 which was filed in June 1992 with the FDA’s Division of Oncology and Pulmonary Drug Products. This IND is now under the purview of the FDA’s Division of Oncology Products. All CMBC studies were conducted under this IND. Miravant kept this IND in place but in 2005 they placed it on inactive status since they had focused their REM-001 development efforts on ophthalmology. In 2012, following St Cloud’s foreclosure action on Miravant and our subsequent purchase of the Miravant assets, St. Cloud transferred ownership of this IND to us. This transfer was formally recognized by the FDA with a Change of Sponsor letter dated December 14, 2012. Our interactions with the FDA for CMBC are under the auspices of this IND. It is our expectation, based on input from regulatory consultants, that clinical development in CMBC, non-CMBC cutaneous metastatic cancer and BCCNS basal cell nevus syndrome would be conducted under this IND. Recent FDA approvals in locally advanced basal cell cancers, which included patients with BCCNS, have been under the purview of the FDA’s Division of Oncology Products.
As part of our purchase agreement with St. Cloud, sponsorship of two other INDs was transferred to us. On February 25, 2013, the FDA’s Division of Dermatology and Dental Products notified us with a Change of Sponsor letter that it recognized us as the sponsor of IND 50,116. On May 8, 2013 the FDA’s Division of Transplant and Ophthalmology Products notified us with a Change of Sponsor letter that it recognized Adgero as the sponsor of IND 49,648. At this time, we do not anticipate any of our planned, or contemplated, clinical development activities would be under either of these INDs.
REM-001 Therapy
Our REM-001 Therapy product consists of three parts, the DD series laser light source (or equivalent), the ML2-0400 light delivery device (or equivalent) and the drug REM-001. Pursuant to the Miravant oncology IND, the FDA previously approved all three components to be used together in certain Miravant CMBC Studies. In use, the drug REM-001 is first administered by intravenous infusion and allowed to distribute within the body and be taken up by the tumors. Tumors are then illuminated with light using the light delivery device, which is attached to the laser light source, so that the accumulated drug REM-001 can be activated for the desired clinical effect. Our analysis of clinical data collected in the Miravant CMBC Studies shows that REM-001 Therapy provides a stronger reaction in tumor tissues than in healthy tissues, which was a goal with REM-001’s formulation.
Our plan is to use new lasers that are functionally equivalent to the Miravant DD2, the laser used in certain prior Miravant clinical studies, for CMBC. The Miravant DD2 lasers are capable of delivering two watts of optical power centered at a wavelength of 664 nanometers. Based on our interactions with the FDA, we believe that use of such new functionally equivalent lasers will be acceptable to the FDA.
The light delivery devices we plan to use in our CMBC program are the same basic design developed and used previously by Miravant in its clinical studies. In the case of cutaneous treatment, such as with CMBC, the light delivery device consists of an optical fiber which has a modified end to allow it to deliver a uniform light treatment field to the tumor. Our plan is to have clinical light delivery devices built by a contract medical device manufacturer using the basic Miravant design and tested to the same performance specifications as used previously.
The REM-001 Drug
REM-001 is a light activated photosensitizer drug used in PDT. During light activation, photosensitizer drugs act as a catalyst and absorb light energy which they transfer to surrounding oxygen-containing molecules to create reactive oxygen species (“ROS”). ROS can initiate various biological mechanisms of action:
|
|
• |
Apoptosis—Certain photosensitizer drugs associate with the cells’ mitochondria. When light activated, these drugs generate ROS that alter mitochondria membrane permeability to allow the release of activators that initiate a programmed cell death process known as apoptosis. Apoptosis is a desirable means of inducing tumor cell death as it is the body’s natural mode for eliminating damaged cells. |
|
|
• |
Necrosis—At higher doses these photosensitizer-generated ROS can overwhelm a cell and induce cellular necrosis. |
15
|
|
• |
Anti-angiogenesis—As they grow, tumors develop their own micro-vasculature network. ROS can be used to create permeability in these micro-vessels which reduces their effectiveness and cuts off the tumor’s blood supply. |
|
|
• |
Immune Response—PDT is known to induce an immune response including activation of CD8+ T cells to attack tumor cells. Such T cells provide one of the key mechanisms making up the body’s immune response system, which response may enhance anti-tumor immunity. Therapeutic drugs that produce such an immune response are known as immunotherapies. We believe that immunotherapies are promising areas of cancer treatment and are being developed as either monotherapies or in combination with other treatments. |
REM-001 has been shown to induce apoptosis and, in treating an aspect of AMD, to have anti-angiogenesis properties. REM-001 is a second-generation photosensitizer drug designed with the following attributes to overcome several of the shortcomings of earlier, first generation photosensitizer drugs such as Photofrin:
|
|
• |
It is activated with longer wavelength, deeper penetrating light; |
|
|
• |
It has a stronger light absorption coefficient; |
|
|
• |
It is a synthetic single molecule; and |
|
|
• |
It causes transient photosensitivity of shorter duration. |
Photofrin, which is sold by Pinnacle Biologics Inc. (“Pinnacle”), a subsidiary of Advanz Pharma Corp (TSX: ADVZ), is the only PDT compound that we are aware of which is approved by the FDA for the treatment of cancer. Specifically, it is approved in the United States for certain non-small-cell lung cancers and esophageal cancers. Currently, Photofrin it is not approved for treatment of CMBC or similar cutaneous tumors and we are not aware of any efforts to get approval in these indications.
REM-001’s chemical structure is designed to allow the use of longer wavelength, deeper penetrating light than is used in Photofrin. Deeper penetrating light means the treatment effect can reach deeper into the tumor which we believe should allow for the treatment of larger tumor volumes. REM-001 also has a stronger light absorption coefficient than Photofrin, which we believe should allow it to generate ROS more efficiently. In addition, REM-001 is an easily synthesized single molecule meaning that its manufacturing process is consistent with modern drug manufacturing strategies; we believe this will make REM-001 better suited for today’s rigorous regulatory environment. Unlike REM-001, Photofrin is a polymer mixture derived from naturally occurring substances. Polymer mixtures can present challenges in achieving a consistent drug product in line with modern regulatory requirements. An additional advantage provided by REM-001 is the rate at which it clears from the skin. Clinical data from a Phase 1 clinical study conducted by Miravant in healthy volunteers showed that, at the 1.2 mg/kg dose of REM-001, there was no measurable photosensitivity when patients were exposed 15 days after drug administration to light equivalent to fifteen minutes of midday sunlight. Further data indicates this effect is present for longer periods if higher drug doses or more extended periods of light exposure are used. Based on our review of limited published data (Wagnieres, et. al., Photochemistry and Photobiology, 1998, 68(3): 382-87), we believe that, when used under similar conditions, the photosensitivity of REM-001 is of shorter duration and is less intense than that seen with Photofrin. In the Wagnieres paper, the authors describe photosensitivity measurements on a human subject that was done using test conditions that were virtually identical to a study conducted by Miravant using REM-001. All patients in the Miravant study had photosensitivity reactions that were much less intense and of much shorter duration than that seen in the Wagnieres paper.
Given what we believe are its potential multiple mechanisms of action, efficacy results to date and substantial development, we believe REM-001Therapy is a promising platform therapy for the treatment of CMBC and other cutaneous metastatic cancers.
REM-001 Safety and Toxicology
PDT carries what we believe is an inherent safety advantage since it uses photosensitizer compounds that are largely inactive except when they are being illuminated by intense light at specific wavelengths. Nevertheless, drug molecules, including photosensitizer molecules, can carry safety or toxicology risks on their own. REM-001 has previously undergone preclinical and clinical studies throughout its development cycle and has undergone certain tests typically required for FDA drug approval. REM-001 has been safely administered to over 1,100 patients in prior clinical studies. Most significantly, REM-001 has been previously reviewed by the FDA as part of the NDA submitted by Miravant for the use of REM-001 to treat an aspect of AMD, a non-CMBC indication. Following that review, the FDA granted an approvable letter for REM-001 in an aspect of AMD in 2004, with final approval contingent on, among other things, the successful completion of a Phase 3 study. While not definitive, we believe this letter, along with feedback we received from FDA meetings, indicates that it is unlikely that there will be significant safety or toxicology issues associated with REM-001 that would ultimately prevent marketing approval.
16
Based on our review of the clinical data of the Miravant CMBC Studies, we believe pain was the most common treatment-related adverse event experienced by patients in these studies. The second most common safety issue experienced with REM-001 was a transient photosensitivity, meaning extended exposure in bright light and direct sunlight should be avoided. Transient photosensitivity occurs with all photosensitizers to some degree. We believe this issue can be addressed by minimizing one’s exposure to bright light and sunlight for two to four weeks after treatment. In general, the potentially treatment-related adverse events observed in these CMBC studies were expected in nature (pain, edema, skin photosensitivity) and severity, and mostly resolved during the course of the studies.
REM-001 Therapy Target Markets
Our development plan for REM-001 Therapy is focused on the treatment of rare unmet needs in cancer, particularly those where the tumor can be accessed with a light delivery fiber device.
CMBC
While most internal cancers can metastasize to the skin, the internal cancer where this most commonly occurs is breast cancer. Radiotherapy is often used as an adjunctive therapy in breast cancer, in part to help prevent the development of local recurrences including CMBC. However, breast cancer survivors may still develop CMBC lesions, even over a decade after their original cancer treatment. In fact, physicians often watch for cutaneous (skin surface) metastases as a sign of breast cancer recurrence. A 2003 meta-analysis of approximately 20,000 cancer patients found that 24% of metastatic breast cancer patients included in the analysis had developed cutaneous metastases, which was the highest rate of skin metastases of any cancer type. Given that approximately 155,000 women suffer from metastatic breast cancer, we believe the prevalence of CMBC may approach 40,000 in the United States. In many cases of CMBC, surgical excision is not possible, so various standard cancer therapies, particularly radiotherapy or chemotherapy, are the first course of treatment. We believe these therapies are inadequate given the well-known dose limiting toxicities, limited efficacy, and/or side effects of each. We are not aware of any prospective clinical studies that have led to FDA approval of a therapy specifically for the treatment of CMBC and we do not expect any to be approved in the near future.
According to an April 2018 market assessment from Charles River Associates, there is an estimated market opportunity of approximately $500 million for the treatment of CMBC.
Cutaneous Metastatic Cancers
A meta-analysis has shown that approximately five percent of people with internal (non-melanoma, non-lymphatic, non-leukemic) cancers develop cutaneous metastatic tumors in their skin. Based on an estimated incidence of 1,500,000 such internal cancers in the United States, this means that the incidence of such cutaneous metastases is approximately 75,000 with a substantially higher prevalence given the fact that individuals often live with metastatic cancer for years. Regardless of the primary source of the cancer, these cutaneous metastatic tumors often begin as small skin nodules but, as the cancer spreads, more nodules form and can eventually cover large areas of skin. With progression, the tumor field generally becomes more painful as tumors may grow larger and more numerous, ulcerate, bleed and carry a strong odor. Part of our goal is to treat these cutaneous tumors as early as possible to either cause them to be locally eliminated or to slow their growth sufficiently to reduce their late stage development.
Basal Cell Carcinoma Nevus Syndrome (“BCCNS”)
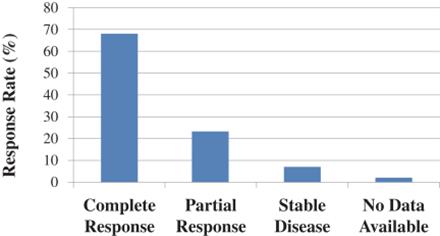
In addition to the clinical studies that Miravant conducted with REM-001 Therapy in CMBC, it also generated clinical data for patients with Basal Cell Carcinoma Nevus Syndrome (“BCCNS”) who developed extensive basal cell carcinoma. BCCNS is a rare but serious condition that is often characterized by the formation of multiple and recurring cutaneous basal cell carcinoma lesions. According to Cancer.net, as of April 2020, approximately 1 in 40,000 individuals in the U.S. have underlying genetic condition that causes BCCNS and approximately 90% of these have BCCNS and it has been recognized as an orphan indication by FDA. In a Miravant Phase 1/2 clinical study (CA001B), 14 patients with BCCNS were enrolled and treated with REM-001 Therapy using the same dosing conditions as were used in the CMBC studies. A total of 157 lesions were treated in these patients and showed a 91% overall response rate. This was composed of a 68% complete response rate (no remaining visible evidence of a lesion) and a 23% partial response rate (lesion was reduced in size by more than 50%). In addition, 7% of lesions had stable disease (any increase in lesion size was less than 25%). The various response rates are shown in the graph below and are similar to the results seen in CMBC patients as we would expect. Based on these results we requested, and were granted, an orphan drug designation for tin ethyl etiopurpurin, the API in REM-001.
17
Until the FDA approval of the drugs Odomzo and Erivedge approximately five and eight years ago, respectively, treatment options for these BCCNS patients were very limited. However, we believe that, based on their package inserts, Odomzo and Erivedge have dose limiting toxicity profiles which are broader in scope than the primarily transient adverse effects observed to-date with REM-001 Therapy. We believe that the potential toxicity limitations related to the existing therapies for BCCNS, plus the positive initial Phase 1/2 data generated in clinical studies with REM-001 Therapy, suggest that REM-001 Therapy could be a viable alternative in treating recurrent basal cell carcinoma in BCCNS patients.
Current and Experimental Treatments for CMBC
As with many cancers, the current standard treatment for CMBC is surgical excision. However, this is often not feasible due to the extent of the tumor field or the condition of the skin, particularly in patients who have had radiation therapy. A number of other therapies have been used on patients with CMBC, including various forms of chemotherapy, radiation therapy, hyperthermia, cryotherapy, electro-chemotherapy, topical drugs and intra-lesional chemotherapy injections. Researchers have also attempted to combine therapies in an effort to improve efficacy. However, we believe that these therapies are often inadequate given the limited efficacy, toxicities and/or side effects of each. The side effects associated with therapies may be particularly difficult for patients who may have already experienced extensive surgery along with a full course of radiation and/or systemic chemotherapy. Also, the fact that CMBC tumors continue to develop following these therapies is a signal that the tumor cells may have developed a resistance to some of these approaches. Based on our discussions with clinicians and literature reviews, and its March 3, 2017 response from FDA, we believe that treatment of unresectable CMBC tumors is a largely unmet medical need, particularly in patients who have already received extensive radiation and chemotherapy.
Clinical Results in CMBC
We have conducted an analysis of the Phase 1 and four Phase 2 and/or Phase 3 CMBC clinical studies done previously with REM-001 Therapy by Miravant (the “Miravant CMBC Studies”) and have concluded that, in these studies, REM-001 Therapy provided higher tumor response rates than are generally seen with alternative CMBC treatments but this program was discontinued in 1998. Our review of Miravant’s records further indicates that, following this decision, Miravant continued to monitor patients in the CMBC studies and collected data as required by protocol, but they conducted no further treatment of CMBC patients with REM-001 Therapy. We believe that Miravant primarily chose to discontinue this program in order to focus its REM-001 development efforts on an aspect of “wet” age-related macular degeneration (“AMD”).
Phase 1 Clinical Study
A Phase 1 dose escalation clinical study was initially conducted by Miravant to establish the REM-001 dosimetry to be used in subsequent safety and efficacy studies. The study was initiated in 1993 and enrolled 22 patients with a variety of types of cutaneous cancer lesions. Of these, 213 cutaneous cancer lesions were treated using escalating REM-001 drug and light doses. This study used earlier generation light delivery devices than those used in later studies but these devices provided equivalent light output to those units used in later studies. In these studies, REM-001 drug doses ranged from 0.1 mg/kg to 1.2 mg/kg, light doses ranged from 100 to 200 J/cm2 and treatment time-points ranged from 24 to 72 hours. This study indicated that a drug dose in excess of 0.8 mg/kg and a light dose of 200 J/cm2 administered at 24 hours provided a high overall response rate when delivered in a variety of cutaneous cancer lesions. The previously tested dose of 1.2mg/kg was then tested further in a second Phase 1 trial, where it was administered to 27 cutaneous tumor lesions and provided a 66% complete response rate and a 90% overall response rate. Based on these results, this dosimetry was used in subsequent CMBC studies, including the Miravant CMBC Studies described below.
18
Phase 2/3 Studies
Miravant conducted four Phase 2/3 studies with REM-001 Therapy for the treatment of CMBC as summarized below. These studies all used the same dosimetry as described above and most of the patients had been previously treated with radiation therapy and chemotherapy. The light delivery devices used in these studies were the ML1-0400 or the functionally equivalent ML2-0400. The laser light source used in three of the studies was the Miravant DD2 laser and one study used the KTP model laser manufactured by LaserScope. Each study was conducted under Miravant’s REM-001 cancer Investigational New Drug Application (“IND”) using Good Clinical Practices with safety and efficacy data collected accordingly. In connection with our acquisition of the Miravant assets, ownership of that IND has been transferred to us.
The table below summarizes the Miravant CMBC Studies. Studies CA008, CA009 and CA019 required that the patients enrolled had received prior radiation therapy. Study CA013 did not have this specific inclusion requirement but our review of the data indicates that at least 50 of the 56 patients in CA013 had received prior radiation therapy. A second difference across the studies is that studies CA008, CA009 and CA019 had a 24-week follow-up period while study CA013 had a 52-week follow-up period. Also, in studies CA008 and CA009 two tumor lesions on each patient were randomly selected as controls and did not receive light activation. CA013 was conducted in Europe by a corporate partner of Miravant. Beyond these differences and those device differences noted above. We believe there were no other substantive differences between the studies and that all studies enrolled similar patients.
Table of Phase 2 and/or 3 Miravant CMBC Studies
(Note: SnET2 is now called REM-001.)
|
Study Title |
|
Phase |
|
|
Location |
|
Total Patients |
|
|
Total Patients Previously Treated with Radiotherapy |
|
|
Included Randomly Selected Control Tumors |
|||
|
CA008: Open-Label Randomized No Treatment Concurrent Controlled Study of Single Dose Tin Ethyl Etiopurpurin (SnET2) Photodynamic Therapy (PDT) in Patients with Advanced Breast Cancer Who Have Failed Radiation Therapy for the Management of Cutaneous Metastatic Breast Carcinoma (24 Week Follow Up) |
|
2/3 |
|
|
U.S. |
|
|
32 |
|
|
|
32 |
|
|
Yes |
|
|
CA009: Open-Label Randomized No Treatment Concurrent Controlled Study of Single Dose Tin Ethyl Etiopurpurin (SnET2) Photodynamic Therapy (PDT) in Patients with Advanced Breast Cancer Who Have Failed Radiation Therapy for the Management of Cutaneous Metastatic Breast Carcinoma (24 Week Follow Up) |
|
2/3 |
|
|
U.S. |
|
|
36 |
|
|
|
36 |
|
|
Yes |
|
|
CA013: Multinational, Open-Label Study of Single Dose Tin Ethyl Etiopurpurin (SnET2) Photodynamic Therapy (PDT) in Patients with Advanced Breast Cancer for the Management of Cutaneous Metastases of Breast Carcinoma (52 Week Follow Up) |
|
|
2 |
|
|
Europe |
|
|
56 |
|
|
|
50 |
|
|
No |
|
CA019: Open-Label Study of Single Dose Tin Ethyl Etiopurpurin (SnET2) Photodynamic Therapy (PDT) in Patients with Advanced Breast Cancer Who Have Failed Radiation Therapy for the Management of Cutaneous Metastatic Breast Carcinoma (24 Week Follow Up) |
|
|
3 |
|
|
U.S. |
|
|
25 |
|
|
|
25 |
|
|
No |
19
The primary endpoints for studies CA008 and CA009 were objective tumor response rate, quality-of-life change, device performance and patient safety. Our review of the tumor response rate and quality-of-life endpoints indicated they were defined as follows:
|
|
• |
Tumor Response: Measured as paired response difference, as calculated by the percentage of a patient’s evaluable lesions that respond minus the percentage of the patient’s control lesions that respond with this difference averaged over all treated patients. |
|
|
• |
Quality of Life Change: Measured using the Dermatologic Life Quality Index (DLQI, A.Y. Finlay and O.K. Khan, “Dermatology Life Quality Index (DLQI—a simple practical measure for routine clinical use”. Clinical and Experimental Dermatology 1994; 19: 210-2 16) with change measured from baseline measurements. |
The following table shows the results of these two endpoints for studies CA008 and CA009 as calculated by Miravant. In some cases, patients dropped out of the study before lesion responses could be assessed or they did not complete their quality of life questionnaires. The Eligible Patients column in this and the following tables refers to the number of patients in each case for which sufficient data is available to calculate the relevant endpoint.
|
|
|
Tumor Response as Measured by Paired Response Endpoint |
|
24 Week Quality of Life Change |
|
|||||||||||||
|
Study |
|
Eligible Patients (N) |
|
|
Mean ± SD (%) |
|
P value |
|
Eligible Patients (N) |
|
|
Mean ± SD |
|
P value |
|
|||
|
CA008 |
|
|
18 |
|
|
33% ± 37% |
|
< 0.001 |
|
|
7 |
|
|
0.4 ± 4.8 |
|
|
0.813 |
|
|
CA009 |
|
|
19 |
|
|
39% ± 47% |
|
< 0.001 |
|
|
10 |
|
|
-0.3 ± 4.1 |
|
|
0.554 |
|
The FDA typically requires a p value of 0.05 or less for approval. Based on the above results, it appears that the Paired Response endpoint achieved statistical significance in both the CA008 and CA009 studies. However, it is our understanding that FDA questions the strength of this data, in part due to the small number of patients involved as well as the fact that each patient had only two control lesions.
Following discussions with the FDA, an endpoint called Clinical Success was added as an additional measure of tumor response. This was defined as follows:
|
|
• |
Clinical Success: Clinical success is determined by a two-step process. First, for each patient, clinical success occurs when the fraction of evaluable lesions that respond minus the fraction of evaluable lesions that progress is greater than 0.5. Second, for the entire study, an average rate of clinical success is determined, simply by taking the ratio of individual patients who are clinical successes to the total number of eligible patients. Note this endpoint does not involve the control lesions or any other control, so a p-value is not appropriate since p-values refer to the difference between a treated and a control group. In such uncontrolled settings, the statistical measure commonly used by regulatory agencies instead of a p-value is the confidence interval, which is provided in the charts below. |
The clinical success rates for studies CA008 and CA009 as calculated by Miravant are provided in the following table:
|
|
|
Tumor Response as Measured by Clinical Success |
||||||||
|
Study |
|
Eligible Patients (N) |
|
|
Average Rate of Clinical Success (%) |
|
|
95% Confidence Interval |
||
|
CA008 |
|
|
20 |
|
|
|
60 |
% |
|
39% - 81% |
|
CA009 |
|
|
20 |
|
|
|
50 |
% |
|
28% - 72% |
No significant device failures were observed in either study. Secondary endpoints in CA008 and CA009 were patient disease burden, duration of response and patient pain assessment. Miravant’s analysis indicated, for patients for which data was available, there was a treatment benefit in disease burden (p = 0.0017 for CA008, p = 0.0020 for CA009) and duration of response (p < 0.001 for CA008, not significant in CA009) when comparing treated and control lesions. In terms of pain, there was no significant change in pain in CA008 and a treatment related increase in pain at 4 Weeks post-treatment in CA009. Treatment related pain, particularly during the first month after treatment, was the most commonly reported adverse event and was often treated with analgesics.
20
Studies CA013 and CA019 used similar endpoints with one notable exception. Tumor Response as Measured by Paired Response was not possible in these studies since this measurement relies on control lesions and CA013 and CA019 did not include controls. Miravant did not conduct an efficacy analysis of these two studies but we have conducted an analysis of the Quality of Life and Clinical Success endpoints used in the pivotal CA008 and CA009 studies. Results from that analysis are shown in the following table:
|
|
|
Clinical Success |
|
24 Week Quality of Life Change |
|
|||||||||||||||
|
Study |
|
Eligible Patients (N) |
|
|
Average Rate of Clinical Success (%) |
|
|
95% Confidence Interval |
|
Eligible Patients (N) |
|
|
Mean ± SD |
|
P value |
|
||||
|
CA013 |
|
|
32 |
|
|
|
88 |
% |
|
71% - 97% |
|
|
16 |
|
|
1.3 ± 3.6 |
|
|
1.00 |
|
|
CA019 |
|
|
18 |
|
|
|
83 |
% |
|
45% - 86% |
|
|
11 |
|
|
2.5 ± 4.7 |
|
|
1.00 |
|
We have not attempted any further analysis of the endpoints included in these two studies.
The most common adverse events seen in these four studies (CA008, CA009, CA013, CA019) were pain and photosensitivity, both of which are expected with this therapy. In the four studies there were a total of 17 serious adverse events (SAE’s) that were judged by investigators to be possibly, probably or definitely related to treatment. None of these were classified by the investigator as life threatening and none resulted in death. Of these, 17 SAE’s, eight were related to necrosis of the treated lesions, three were related to treatment field infection, 4 were treatment related pain, one was a photosensitivity skin reaction and one was an allergic reaction.
We believe that the data from these studies show that REM-001 Treatment is a promising therapy for CMBC. However, because there are no approved therapies for CMBC, we have no basis for comparing these results to existing therapies. Based on the FDA’s March 3, 2017 response, we believe the FDA will view these results as supportive data and our plan is to conduct a new pivotal Phase 3 study to support a new drug application.
The figure below shows the results of this initial preliminary analysis of Miravant clinical data and depicts the percentage of evaluable lesions in each Miravant CMBC Study for which there was a complete response; i.e. where all visible clinical evidence of the tumor is gone after treatment with REM-001 Therapy.
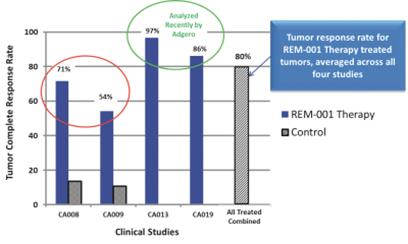
Clinical Development Plans
CMBC
Our initial product goal is to achieve marketing approval of REM-001 Therapy for the treatment of CMBC. We conducted a preliminary analysis of existing REM001 Therapy clinical study data for CMBC from the Miravant CMBC Studies. This analysis was overseen by regulatory experts who have expertise in interacting with the Food and Drug Administration (the “FDA”). The consultants we have engaged are either former FDA employees with directly related experience in reviewing similar oncology treatments who are now acting as independent consultants or individuals who have provided senior regulatory guidance to major pharmaceutical or medical device companies in situations that led to regulatory approval. For this first analysis, we had submitted questions to FDA under a Type C format to review the technology and results and determine the anticipated requirements for regulatory approval. On March 3, 2017, we received FDA’s written response to our questions. Based on that response, we believe our
21
plans to manufacture REM-001 by revising the prior quality standards to meet the currently recommended regulatory standards will be acceptable. The FDA also indicated our plans for utilizing light delivery devices that have been shown to be functionally equivalent to the devices used by Miravant will be acceptable. In October 2017, we held a Type B face-to-face guidance meeting with the FDA that was primarily focused on the design of a Phase 3 study in CMBC. In May 2018, we held a Type B end-of-phase 2 meeting with the FDA that focused on our plans for addressing CMC and device topics related to our CMBC effort. In these interactions the FDA provided guidance on a number of clinical parameters they would like us to measure in our planned clinical study and on our CMC and device plans. Based on FDA’s responses, our plan is to conduct a Phase 3 clinical study in CMBC to test the safety and efficacy of REM-001 Therapy for marketing approval. In June 2018, we submitted to FDA a Phase 3 protocol and statistical analysis plan incorporating feedback received from the FDA at our October 2017 meeting. We have also undertaken extensive discussions with clinical research organizations to carry out this study and has received detailed proposals from five of these organizations. Since our May 2018 meeting, we have engaged a contract manufacturer who has manufactured the starting material for our active pharmaceutical ingredient (API), manufactured two API lots under GMP and has stability testing underway. We are currently working to undertake GMP manufacture of finished drug product for use in our clinical study.
At this time, we estimate the necessary study design will be a pivotal Phase 3 multi-center study that would enroll approximately 100-150 CMBC patients who have received prior radiation therapy and chemotherapy. This study has been designed with input from the FDA with the goal of gaining expedited development and review through one or more of the FDA’s expedited programs. Following our meeting with the FDA, we undertook further analysis of the original Miravant study data and concluded that the data may support use of a lower dose than Miravant used in its original study design. Use of such a lower dose may have potential benefits including faster post-treatment healing and response assessment and lower drug exposure. Based on this analysis and discussions with regulatory and clinical consultants, including prior FDA employees or consultants, and clinical research organizations, we plan to add a preliminary confirmatory element to our Phase 3 study. This confirmatory element anticipates treating up to 15 patients at a lower dose than used by Miravant. Patients treated in this confirmatory phase will not be included in the pivotal study efficacy population but their results should provide an indication that a lower dose may be as effective as the original Miravant dose and they may be used to provide a further preliminary confirmation of the potential of REM-001 Therapy in CMBC and if the results are sufficiently compelling we may use them as guidance for the use of a slightly lowered dose in the pivotal study. This confirmatory phase was included in the protocol submitted to FDA in June 2018 and we have not received comment on this from FDA although based on guidance from our regulatory consultants we believe the FDA will be supportive of this design.
We have also been in ongoing discussions with the FDA seeking an orphan drug designation for REM-001 in the treatment of CMBC. Our research indicates that CMBC prevalence is less than 200,000 in the United States, thus we believe we should qualify for an orphan drug designation. However, to-date, the FDA has not accepted this rationale. At this time, we can offer no assurances that FDA will grant an orphan drug designation for REM-001 in CMBC. Our request is based on existing clinical data in CMBC patients. The FDA also grants five years data of exclusivity to the first applicant to obtain approval of an NDA for a new chemical entity (“NCE”). A drug is an NCE if the FDA has not previously approved any other new drug containing the same active ingredient. We believe that REM-001 would also qualify for this form of exclusivity. There is no guarantee that we will receive an orphan drug designation or NCE exclusivity for REM-001.
Manufacturing
VAL-083
VAL-083 is a small-molecule chemotherapeutic. Chemical synthesis of the active pharmaceutical ingredient (“API”) was initially established by the NCI. We have made improvements to this process and have obtained patents on these improvements. The current manufacturing process involves fewer than five synthetic steps.
VAL-083 drug product is a lyophilized (freeze-dried) formulation that is reconstituted for intravenous injection. We anticipate that overall cost of goods for an eventual commercial product will be similar to other injectable, small-molecule pharmaceuticals.
For our clinical study being conducted in China, the supply of VAL-083 has been provided through our collaboration with Guangxi Wuzhou Pharmaceutical Company. Guangxi Wuzhou Pharmaceutical Company as a manufacturer has established a commercial-scale manufacturing process based on the North American process originally developed for the NCI that has been licensed by the CFDA for commercial supply of VAL-083 in China. However, to-date, they have not achieved the quality of systems necessary to meet FDA manufacturing standards.
To address the need to meet FDA standards, we have engaged third-party contract manufacturers with the capabilities to establish the processes, procedures and quality systems necessary to meet U.S., Canadian, E.U. and other international manufacturing requirements in accordance with Good Manufacturing Practice (“cGMP”) regulations. We have now received drug supply manufactured under full cGMP conditions. We intend to use this drug supply for all future clinical studies.
22
We have developed and patented certain intellectual property related to quality controls that are used in the release of VAL-083 for our clinical studies in the United States. This intellectual property is also required for product release under CFDA guidelines and we have granted access to our intellectual property for this purpose.
REM-001
The manufacturing process for the API in REM-001 was developed over a ten-year period and we believe is now well established and suitable for commercial scale production. This process was also included as part of Miravant’s prior NDA for the use of REM-001 to treat an aspect of AMD, which underwent an FDA review where an approvable letter was granted. The final REM-001 drug product is a lipid-based formulation and was previously produced at a commercial scale by a contract manufacturer for use in Miravant’s past clinical studies and commercialization activities. We do not own or operate manufacturing facilities for the production of REM-001, nor the laser light source, light delivery device for use with REM-001 Therapy. We will depend on third-party suppliers and manufacturing organizations for both commercial and clinical study supplies of all of our raw materials, the REM-001 drug substance, drug product and the REM-001 Therapy, laser light source, and light delivery device. We have engaged a contract manufacturer who has manufactured the starting material for our API and then manufactured two API lots under GMP and has stability testing underway. We are currently working to finalize agreements with a GMP manufacturer of finished drug product for use in our planned clinical study. With the feedback from the FDA that we could utilize the existing supply of laser systems or devices that were functionally equivalent, an in-depth assessment was made to determine which pathway would be appropriate. It has been determined that the existing lasers that were utilized in the previous clinical studies will not be used in the current clinical studies. We have identified several laser manufactures that could be used as third-party contract medical product manufacturers to build new units, train the clinical staff in the use of the units, provide regulatory support for the devices, and maintain the devices while being used in the study. In the case of the light delivery device, we will also need to obtain these from a third-party contract medical device manufacturer and a supplier has been identified. We believe there are readily available supplies of all raw materials needed for the manufacture of REM-001 and the related required light device components.
Research and Development Collaborations
Guangxi Wuzhou Pharmaceutical Company
Pursuant to a memorandum of understanding and collaboration agreement, dated October 25, 2012, we have established a strategic collaboration with Guangxi Wuzhou Pharmaceutical Company, a subsidiary of publicly traded Guangxi Wuzhou Zhongheng Group Co., Ltd. (SHG: 600252) (the “Guangxi Agreement”). VAL-083 is approved for the treatment of chronic myelogenous leukemia (“CML”) and lung cancer in China and Guangxi Wuzhou Pharmaceutical Company is the only manufacturer licensed by the CFDA to produce the product for the China market. Through the Guangxi Agreement, we have been provided drug product for our ongoing Phase 2 study in China as well as for certain clinical studies in the United States. In addition, we have secured certain commercial rights in China.
Pursuant to the Guangxi Agreement, we have granted to Guangxi Wuzhou Pharmaceutical Company a royalty-free license to certain of our intellectual property for use in China as it relates to quality control and drug production methods for VAL-083. In addition, subject to successful agreement on definitive commercial terms, we have agreed that Guangxi Wuzhou Pharmaceutical Company will be our exclusive supplier of VAL-083 for clinical studies and commercial sales, subject to Guangxi Wuzhou Pharmaceutical Company obtaining and maintaining cGMP certification by the FDA, EMA or other applicable regulatory agencies, and Guangxi Wuzhou Pharmaceutical Company being able to meet volumes ordered by us. To-date, Guangxi Wuzhou Pharmaceutical Company has not achieved cGMP certification with respect to the manufacturing of VAL-083.
This Guangxi Agreement also provides us with certain exclusive commercial rights related to drug supply. Specifically, the Guangxi Agreement establishes an exclusive supply relationship between us and Guangxi Wuzhou Pharmaceutical Company for the Chinese market and all markets outside China. Guangxi Wuzhou Pharmaceutical Company agreed that it may not sell VAL-083 for markets outside of China to any other purchaser other than us, provided that, during the first three years following regulatory clearance for marketing of VAL-083 in a particular country or region, we meet proposed sales volumes set by Guangxi Wuzhou Pharmaceutical Company for the country or region. In addition, Guangxi Wuzhou Pharmaceutical Company granted us a pre-emptive right in China (subject to our acceptance of proposed sales volume and prices) to purchase VAL-083 produced by Guangxi Wuzhou Pharmaceutical Company.
With respect to the Phase 3, or registration study, for GBM to be undertaken in China in order to ultimately commercialize VAL-083 in China, we are not under an obligation to participate in such a study. However, our participation in such a study in China, for the Chinese market, would be part of a larger negotiation process between us and Guangxi Wuzhou Pharmaceutical Company to determine how such a study would be conducted. We plan to execute a Phase 3 study and to seek approval for VAL-083 outside of China and we have no dependency or obligations to Guangxi Wuzhou Pharmaceutical Company with respect to studies we plan to conduct outside of China.
23
The term of the Guangxi Agreement (except as it relates to the exclusive rights in the China market) is indefinite, subject to termination upon written agreement of all parties, or if either party breaches any material term and fails to remedy such breach within 30 days of receipt of notice of the breach, or if any action to be taken thereunder is not agreed to by both parties, provided that such matter is referred to the chief executive officer of both parties, and they are unable to resolve such matter within 90 days. No payments have been made to date under the Guangxi Agreement to, or from, either Kintara or Guangxi Wuzhou Pharmaceutical Company.
St. Cloud Asset Purchase Agreement
Adgero acquired certain Miravant assets, including the REM-001 Therapy and the associated technology and intellectual property, through an asset purchase agreement with St. Cloud Investments, LLC (“St. Cloud”), dated November 26, 2012, as amended (the “St. Cloud Agreement”). In conjunction with the merger with Adgero which closed on August 19, 2020, we assumed the St. Cloud Agreement. St. Cloud was previously a Miravant creditor and acquired these Miravant assets pursuant to a foreclosure process St. Cloud completed under California law. Pursuant to the terms of the St. Cloud Agreement, we are obligated to make certain payments under the agreement. The amounts paid or owed under that agreement are as follows:
|
|
• |
Thirteen thousand dollars ($13,000) was paid to Steven Rychnovsky, PhD, our Vice President, Research and Development, upon the initial closing of an Adgero private placement conducted in 2016 (the “2016 Private Placement”). |
|
|
• |
Forty thousand dollars ($40,000) was paid to St. Cloud upon the initial closing of the 2016 Private Placement. |
|
|
• |
Fifty thousand dollars ($50,000) was paid to Steven Rychnovsky, PhD during the 2016 Private Placement, because the 2016 Private Placement was completed for an amount that exceeded four million dollars ($4,000,000). |
|
|
• |
Fifty thousand dollars ($50,000) was paid to St. Cloud during the 2016 Private Placement, because the 2016 Private Placement was completed for an amount that exceeded four million dollars ($4,000,000). |
|
|
• |
Upon the earlier of (i) a subsequent equity financing to take place after we conduct a Phase 2B clinical study in which fifty patients complete the study and their clinical data can be evaluated or (ii) the commencement of a clinical study intended to be used as a definitive study for market approval in any country, we are obligated to pay an aggregate amount of three hundred thousand dollars ($300,000) in cash or an equivalent amount of common stock, with two hundred forty thousand dollars ($240,000) to St. Cloud and sixty thousand dollars ($60,000) to Steven Rychnovsky, PhD. |
|
|
• |
Upon receipt of regulatory approval of REM-001 Therapy, we are obligated to pay an aggregate amount of seven hundred thousand dollars ($700,000) in cash or an equivalent amount of common stock, with five hundred and sixty thousand dollars ($560,000) to St. Cloud and one hundred forty thousand dollars ($140,000) to Steven Rychnovsky, PhD. |
With respect to the $300,000 and $700,000 potential milestone payments referenced above (each a “Milestone Payment”), if either such Milestone Payment becomes payable, and in the event we elect to pay either such Milestone Payment in shares of our common stock, the value of the common stock will equal the price per share of the most recent financing, or, if we are considered to be a publicly-traded company, the average of the closing price per share of our common stock over the twenty (20) trading days following the first public announcement of the applicable event described above.
In addition, we must pay to St. Cloud and Steven Rychnovsky, PhD, in the aggregate, a royalty fee of six percent (6%) of net sales during the royalty term on a country-by-country and product-by-product basis with St. Cloud receiving a royalty rate of four and eight tenths percent (4.8%) and Steven Rychnovsky, PhD, receiving a royalty of one and two tenths percent (1.2%). The royalty term for a product commences on the first commercial sale of the product, such as REM-001 Therapy, in any country, and the royalty fee must be paid within 30 days of each calendar quarter during which revenue is collected. The royalty term terminates on the later of (i) the invalidation, revocation, lapse or expiration of the last to expire valid claim on any patent acquired in the St. Cloud Agreement that would be infringed by the sale of the product in the country where the commercial sale takes place or (ii) the expiration of the period for which we hold exclusive marketing rights of the product in the country, if we were granted those rights under the St. Cloud Agreement.
Patents and Proprietary Rights
Our success will depend in part on our ability to protect our existing product candidates and the products we acquire or license by obtaining and maintaining a strong proprietary position. To develop and maintain our position, we intend to continue relying upon the validity and enforceability of our patents patent protection, orphan drug status, Hatch-Waxman exclusivity, trade secrets, know-how, continuing technological innovations and licensing opportunities.
There is no guarantee that patents will be granted with respect to any patent applications we may submit, own or license in the future, nor can we be sure that any of our existing patents or any patents we may own or license in the future will be useful in protecting our technology.
24
VAL-083
We have filed patent applications claiming the use of, and improvements related to VAL-083. Our patent filings also include proposed treatment regimens, improvements to the manufacturing process, formulation and composition of the active pharmaceutical ingredient, and finished dosage forms of VAL-083. We are prosecuting our patent applications in the United States and other jurisdictions which we deem important for the potential commercial success of VAL-083.
Our patents and patent applications for VAL-083 can be summarized in fourteen series as follows:
|
|
• |
Series I is generally directed to synthesis of VAL-083. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent No. 8,563,758 |
|
Method Of Synthesis Of Substituted Hexitols Such As Dianhydrogalactitol |
|
|
|
United States Patent No. 8,921,585 |
|
Method Of Synthesis Of Substituted Hexitols Such As Dianhydrogalactitol |
|
|
|
United States Patent No. 9,085,544 |
|
Method Of Synthesis Of Substituted Hexitols Such As Dianhydrogalactitol |
|
|
|
United States Patent No. 9,630,938 |
|
Method Of Synthesis Of Substituted Hexitols Such As Dianhydrogalactitol |
|
|
|
PCT Patent Application Serial No. PCT/US2011/048032 |
|
Method Of Synthesis Of Substituted Hexitols Such As Dianhydrogalactitol. National phase applications pending and granted in various countries. |
|
2031 |
|
|
• |
Series II is generally directed to use of VAL-083 to treat a range of diseases and conditions, including but not limited to malignancies. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent No. 9,066,918 |
|
Compositions And Methods To Improve The Therapeutic Benefit Of Suboptimally Administered Chemical Compounds Including Substituted Hexitols Such As Dianhydrogalactitol And Diacetyldianhydrogalactitol |
|
|
|
United States Patent No. 9,901,563 |
|
Compositions And Methods To Improve The Therapeutic Benefit Of Suboptimally Administered Chemical Compounds Including Substituted Hexitols Such As Dianhydrogalactitol And Diacetyldianhydrogalactitol |
|
|
|
|
• |
Series III is generally directed to analytical methods for VAL-083. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent No. 9,759,698 |
|
Improved Analytical Methods For Analyzing And Determining Impurities In Dianhydrogalactitol |
|
|
|
United States Patent No. 10,145,824 |
|
Improved Analytical Methods For Analyzing And Determining Impurities In Dianhydrogalactitol |
|
|
|
United States Patent No. 9,029,164 |
|
Improved Analytical Methods For Analyzing And Determining Impurities In Dianhydrogalactitol |
|
|
|
PCT Patent Application Serial No. PCT/IB2013/000793 |
|
Improved Analytical Methods For Analyzing And Determining Impurities In Dianhydrogalactitol. National phase applications pending and granted in various countries. |
|
2033 |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
PCT Patent Application Serial No. PCT/US2014/066087 |
|
Improved Analytical Methods For Analyzing And Determining Impurities In Dianhydrogalactitol. |
|
2034 |
25
|
|
• |
Series IV is generally directed to the use of VAL-083 to treat GBM or medulloblastoma. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 16/242,752 |
|
Use Of Substituted Hexitols Including Dianhydrogalactitol And Analogs To Treat Neoplastic Disease And Cancer Stem Cells Including Glioblastoma Multiforme And Medulloblastoma |
|
|
|
United States Patent No. 9,687,466 |
|
Use Of Substituted Hexitols Including Dianhydrogalactitol And Analogs To Treat Neoplastic Disease And Cancer Stem Cells Including Glioblastoma Multiforme And Medulloblastoma |
|
|
|
United States Patent No. 10,201,521 |
|
Use Of Substituted Hexitols Including Dianhydrogalactitol And Analogs To Treat Neoplastic Disease And Cancer Stem Cells Including Glioblastoma Multiforme And Medulloblastoma |
|
|
|
PCT Patent Application Serial No. PCT/US2013/022505 |
|
Use Of Substituted Hexitols Including Dianhydrogalactitol And Analogs To Treat Neoplastic Disease And Cancer Stem Cells Including Glioblastoma Multiforme And Medulloblastoma. National phase applications pending in various countries. |
|
2033 |
|
|
• |
Series V is generally directed to the veterinary use of VAL-083. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent No. 9,814,693 |
|
Veterinary Use Of Dianhydrogalactitol, Diacetyldianhydrogalactitol, And Dibromodulcitol To Treat Malignancies |
|
|
|
|
• |
Series VI is generally directed to the use of VAL-083 to treat tyrosine-kinase-inhibitor-resistant malignancies. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 14/409,909 |
|
Methods For Treating Tyrosine-Kinase-Inhibitor-Resistant Malignancies In Patients With Genetic Polymorphisms Or Ahi1 Dysregulations Or Mutations Employing Dianhydrogalactitol, Diacetyldianhydrogalactitol, Dibromodulcitol, Or Analogs Or Derivatives Thereof |
|
|
|
PCT Patent Application Serial No. PCT/US2013/047320 |
|
Methods For Treating Tyrosine-Kinase-Inhibitor-Resistant Malignancies In Patients With Genetic Polymorphisms Or Ahi1 Dysregulations Or Mutations Employing Dianhydrogalactitol, Diacetyldianhydrogalactitol, Dibromodulcitol, Or Analogs Or Derivatives Thereof. National phase applications pending in various countries. |
|
2033 |
|
|
• |
Series VII is generally directed to the use of VAL-083 to treat recurrent malignant glioma and progressive secondary brain tumor. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 14/682,226 |
|
Use Of Dianhydrogalactitol And Analogs And Derivatives Thereof To Treat Recurrent Malignant Glioma Or Progressive Secondary Brain Tumor |
|
|
|
PCT Application Serial No. PCT/US2014/040461 |
|
Use Of Dianhydrogalactitol And Analogs And Derivatives Thereof To Treat Recurrent Malignant Glioma Or Progressive Secondary Brain Tumor. National phase applications pending and granted in various countries. |
|
2034 |
26
|
|
• |
Series VIII is generally directed to the use of VAL-083 to treat non-small-cell lung cancer. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 14/710,240 |
|
Use of Dianhydrogalactitol and Analogs or Derivatives Thereof in Combination With Platinum-Containing Antineoplastic Agents to Treat Non Small-Cell Carcinoma of the Lung and Brain Metastases |
|
|
|
PCT Patent Application Serial No. PCT/US2015/024462 |
|
Use of Dianhydrogalactitol and Analogs or Derivatives Thereof to Treat Non-Small Cell Carcinoma of the Lung and Ovarian Cancer. National phase applications pending in various countries. |
|
2035 |
|
|
• |
Series IX is generally directed to the use of VAL-083 and radiation to treat NSCLC and GBM. |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 15/525,933 |
|
Dianhydrogalactitol Together with Radiation to Treat Non-Small-Cell Carcinoma of the Lung and Glioblastoma Multiforme. |
|
|
|
PCT Patent Application Serial No. PCT/US2015/059814 |
|
Dianhydrogalactitol Together with Radiation to Treat Non-Small-Cell Carcinoma of the Lung and Glioblastoma Multiforme. National phase applications pending in various countries. |
|
2035 |
|
|
• |
Series X is generally directed to the use of VAL-083 in NSCLC and ovarian cancer: |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 15/759,104 |
|
Use of Dianhydrogalactitol And Derivatives Thereof in the Treatment of Glioblastoma, Lung Cancer and Ovarian Cancer. |
|
|
|
|
• |
Series XI is generally directed to the use of VAL-083 in the treatment of CNS malignancies: |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 15/771,631 |
|
Use of Dianhydrogalactitol or Derivatives and Analogs Thereof for Treatment of Pediatric Central Nervous System Malignancies. |
|
|
|
|
• |
Series XII is generally directed to the analysis and resolution of VAL-083 preparations: |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 10,591,445 |
|
Methods for analysis and Resolution of Preparations of Dianhydrogalactitol and Derivatives and Analogs Thereof. |
|
|
|
United States Patent Application Serial No. |
|
Methods for analysis and Resolution of Preparations of Dianhydrogalactitol and Derivatives and Analogs Thereof. |
|
2036 |
|
PCT Patent Application Serial No. |
|
Methods for analysis and Resolution of Preparations of Dianhydrogalactitol and Derivatives and Analogs Thereof. National phase applications pending in various countries. |
|
|
|
|
• |
Series XIII is generally directed to combinations: |
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. |
|
Use of Dianhydrogalactitol and Analogs and Derivatives in Combination VEGF inhibitors to Treat Cancer |
|
|
|
PCT Patent Application Serial No. PCT/US2018/030391 |
|
Use of Dianhydrogalactitol and Analogs and Derivatives in Combination VEGF inhibitors to Treat Cancer National phase applications pending in various countries. |
|
2038 |
27
|
Patent or Patent Application No. |
|
Title |
|
Expiry |
|
United States Patent Application Serial No. 16/768,827 |
|
Use of Dianhydrogalactitol and Analogs and Derivatives in Combination with a P53 Modulator or a PARP Inhibitor |
|
2038 |
One of the inventors listed in our Series IX applications is an employee of the University of California, San Francisco. If a patent issues from a patent application in this series with a claim that the University of California employee conceived of, in whole or in part, then the Regents of the University of California will share ownership of any such patent with us. Our research agreements with the University of California address this issue by providing us with an exclusive option, for a limited period of time, to negotiate a royalty-bearing exclusive license for commercialization of the invention covered by that patent.
In addition to patent protection, we may also seek orphan drug status whenever it is available. If a product which has an orphan drug designation subsequently receives the first regulatory approval for the indication for which it has such designation, the product is entitled to orphan exclusivity, meaning that the applicable regulatory authority may not approve any other applications to market the same drug for the same indication, except in very limited circumstances, for a period of seven years in the U.S. and Canada, and 10 years in the E.U. Orphan drug designation does not prevent competitors from developing or marketing different drugs for the same indication or the same drug for a different clinical indication.
VAL-083 has been granted protection under the Orphan Drug Act by the FDA and the European Medicines Agency for the treatment of gliomas, including GBM. The FDA has also granted Orphan Drug protection to VAL-083 for the treatment of medulloblastoma and ovarian cancer.
In February 2012, the FDA granted orphan drug status to VAL-083 for the treatment of glioma. In January 2013, the EMA also granted orphan drug protection to VAL-083 for the treatment of glioma. In the spring of 2016, the FDA Office of Orphan Products Development granted orphan drug designations to VAL-083 for the treatment of ovarian cancer and medulloblastoma.
In addition to our patents and orphan drug protection, we intend to rely on the Hatch-Waxman Amendments for five years of data exclusivity for VAL-083.Under the Hatch-Waxman Amendments, newly approved drugs and indications benefit from a statutory period of non-patent marketing exclusivity. These amendments provide five-year data exclusivity to the first applicant to gain approval of an NDA for a new chemical entity, meaning that the FDA has not previously approved any other new drug containing the same active ingredient. The Hatch-Waxman Amendments prohibit the approval of an abbreviated new drug application, also known as an ANDA or generic drug application, during the five-year exclusive period if no patent is listed. If there is a patent listed and the ANDA applicant certifies that the NDA holder’s listed patent for the product is invalid or will not be infringed, the ANDA can be submitted four years after NDA approval. Protection under the Hatch-Waxman Amendments will not prevent the filing or approval of another full NDA; however, the applicant would be required to conduct its own pre-clinical studies and adequate and well-controlled clinical studies to demonstrate safety and effectiveness. The Hatch-Waxman Amendments also provide three years of data exclusivity for the approval of NDAs with new clinical studies for previously approved drugs and supplemental NDAs, for example, for new indications, dosages or strengths of an existing drug, if new clinical investigations were conducted by or on behalf of the sponsor and were essential to the approval of the application. This three-year exclusivity covers only the new changes associated with the supplemental NDA and does not prohibit the FDA from approving ANDAs for drugs containing the original active ingredient.
We also rely on trade secret protection for our confidential and proprietary information. We believe that the substantial costs and resources required to develop technological innovations, such as the manufacturing processes associated with VAL-083, will help us to protect the competitive advantage of our product candidate.
The protection of intellectual property rights in China (where VAL-083 is manufactured pursuant to a collaboration agreement with the only manufacturer presently licensed by the CFDA to produce the product for the China market, and where VAL-03 is approved for the treatment of CML and lung cancer) is relatively weak compared to the United States, which may negatively affect our ability to generate revenue from VAL-083 in China.
Our policy is to require our employees, consultants, outside scientific collaborators, sponsored researchers and other advisors to execute confidentiality agreements upon the commencement of employment or consulting relationships with us. These agreements provide that all confidential information developed or made known to the individual during the course of the individual’s relationship with us is to be kept confidential and not disclosed to third parties except in specific circumstances. In the case of employees and consultants, the agreements provide that all inventions conceived by the individual shall be our exclusive property.
28
REM-001
Our intellectual property and product pipeline for REM-001 is based on technology we acquired that was originally developed by Miravant. We acquired this intellectual property through an asset purchase agreement and our retention of the intellectual property is dependent on us meeting the terms of that agreement, most of which are milestone and royalty-based payments. The acquired intellectual property includes scientific and regulatory data, product know-how and eight issued US Utility patents, some of which have expired or are nearing expiration. Two of the patents contain process claims that pertain specifically to REM-001 and its production with one of these having expired in August 2020 and the other set to expire in March 2021. Two of the patents are for light delivery devices intended to deliver light to internal body surfaces. The first of these having device and process claims expired in August 2020. The other has device claims and is set to expire in September 2024. Of the other four patents, two contain method of use claims that pertain to cardiovascular PDT with one of these set to expire in November 2021 and the other set to expire in May 2021. The one remaining patent is a composition of matter patent for a next generation photosensitizer drugs that we believe may be useful in a range of diseases and is set to expire in November 2021. The proprietary regulatory data we own includes two INDs for use of REM-001 in oncology and ophthalmology, and one NDA for use of REM-001 to treat an aspect of AMD.
We do not hold any patents covering the DD series laser light source or the ML2-0400 light delivery device. However, we believe there are readily available market supplies of lasers and related required light device components for use in our planned studies.
The FDA granted our request that tin ethyl etiopurpurin (the active pharmaceutical ingredient in REM-001) be designated as an orphan drug for treatment of BCCNS. We also hold an orphan drug designation that was initially awarded to Miravant for tin ethyl etiopurpurin for the prevention of access graft disease in hemodialysis patients.
Government Regulation and Product Approval
Regulation by governmental authorities in the U.S. and other countries is a significant factor, affecting the cost and time of our research and product development activities, and will be a significant factor in the manufacture and marketing of any approved products. Our product candidates will require regulatory approval by governmental agencies prior to commercialization. In particular, our products are subject to rigorous preclinical and clinical testing and other approval requirements by the FDA and similar regulatory authorities in other countries. Various statutes and regulations also govern or influence the manufacturing, safety, reporting, labeling, transport and storage, record keeping and marketing of our products. The lengthy process of seeking these approvals, and the subsequent compliance with applicable statutes and regulations, require the expenditure of substantial resources. Any failure by us to obtain, or any delay in obtaining, the necessary regulatory approvals could harm our business.
The regulatory requirements relating to the testing, manufacturing and marketing of our products may change from time to time and this may impact our ability to conduct clinical studies and the ability of independent investigators to conduct their own research with support from us.
The clinical development, manufacturing and marketing of our products are subject to regulation by various authorities in the U.S., the E.U. and other countries, including, in the U.S., the FDA, in Canada, Health Canada, and, in the E.U., the EMA. The Federal Food, Drug, and Cosmetic Act, the Public Health Service Act in the U.S. and numerous directives, regulations, local laws and guidelines in Canada and the E.U. govern the testing, manufacture, safety, efficacy, labeling, storage, record keeping, approval, advertising and promotion of our products. Product development and approval within these regulatory frameworks takes a number of years and involves the expenditure of substantial resources.
Regulatory approval will be required in all the major markets in which we seek to develop our products. At a minimum, approval requires the generation and evaluation of data relating to the quality, safety, and efficacy of an investigational product for its proposed use. The specific types of data required and the regulations relating to this data will differ depending on the territory, the drug involved, the proposed indication and the stage of development.
In general, new chemical entities are tested in animals until adequate evidence of safety is established to support the proposed clinical study protocol designs. Clinical studies for new products are typically conducted in three sequential phases that may overlap. In Phase 1, the initial introduction of the pharmaceutical into either healthy human volunteers or patients with the disease (20 to 50 subjects), the emphasis is on testing for safety (adverse effects), dosage tolerance, metabolism, distribution, excretion and clinical pharmacology. Phase 2 involves studies in a limited patient population (50 to 200 patients) to determine the initial efficacy of the pharmaceutical for specific targeted indications, to determine dosage tolerance and optimal dosage and to identify possible adverse side effects and safety risks. Once a compound shows preliminary evidence of some effectiveness and is found to have an acceptable safety profile in Phase 2 evaluations, Phase 3 studies are undertaken to more fully evaluate clinical outcomes in a larger patient population in adequate and well-controlled studies designed to yield statistically sufficient clinical data to demonstrate efficacy and safety.
29
In the U.S., specific preclinical data, manufacturing and chemical data, as described above, need to be submitted to the FDA as part of an IND application, which, unless the FDA objects, will become effective 30 days following receipt by the FDA. Phase 1 studies in human volunteers may commence only after the application becomes effective. Prior regulatory approval for human healthy volunteer studies is also required in member states of the E.U. Currently, in each member state of the E.U., following successful completion of Phase 1 studies, data are submitted in summarized format to the applicable regulatory authority in the member state in respect of applications for the conduct of later Phase 2 studies. The regulatory authorities in the E.U. typically have between one and three months in which to raise any objections to the proposed study, and they often have the right to extend this review period at their discretion. In the U.S., following completion of Phase 1 studies, further submissions to regulatory authorities are necessary in relation to Phase 2 and 3 studies to update the existing IND.
Authorities may require additional data before allowing the studies to commence and could demand that the studies be discontinued at any time if there are significant safety issues. In addition to the regulatory review, studies involving human subjects must be approved by an independent body. The exact composition and responsibilities of this body will differ from country to country. In the U.S., for example, each study will be conducted under the auspices of an independent institutional review board (IRB) at each institution at which the study is conducted. The IRB considers among other things, the design of the study, ethical factors, the privacy of protected health information as defined under the Health Insurance Portability and Accountability Act, the safety of the human subjects and the possible liability risk for the institution. Equivalent rules to protect subjects’ rights and welfare apply in each member state of the E.U. where one or more independent ethics committees, which typically operate similarly to an IRB, will review the ethics of conducting the proposed research. Other regulatory authorities around the rest of the world have slightly differing requirements involving both the execution of clinical studies and the import/export of pharmaceutical products. It is our responsibility to ensure we conduct our business in accordance with the regulations of each relevant territory.
In order to gain marketing approval, we must submit a dossier to the relevant authority for review, which is known in the U.S. as a new drug application (NDA) and in the E.U. as a marketing authorization application (MAA). The format is usually specific and laid out by each authority, although in general it will include information on the quality of the chemistry, manufacturing and pharmaceutical aspects of the product as well as the nonclinical and clinical data. Once the submitted NDA is accepted for filing by the FDA, it undertakes the review process that currently takes on average 10 months, unless an expedited priority review is granted which takes six months to complete. Approval can take several months to several years, if multiple 10-month review cycles are needed before final approval is obtained, if at all.
The approval process can be affected by a number of factors. The NDA may require additional preclinical, manufacturing data or clinical studies which may be requested at the end of the 10-month NDA review cycle, thereby delaying approval until additional data are submitted and may involve substantial unbudgeted costs.
In addition to obtaining approval for each product, in many cases each drug manufacturing facility must be approved. The regulatory authorities usually will conduct an inspection of relevant manufacturing facilities, and review manufacturing procedures, operating systems and personnel qualifications. Further inspections may occur over the life of the product. An inspection of the clinical investigation sites by a competent authority may be required as part of the regulatory approval procedure. As a condition of marketing approval, the regulatory agency may require post-marketing surveillance to monitor for adverse effects or other additional studies as deemed appropriate. After approval for the initial indication, further clinical studies may be necessary to gain approval for any additional indications. The terms of any approval, including labeling content, may be more restrictive than expected and could affect the marketability of a product.
The FDA offers a number of regulatory mechanisms that provide expedited or accelerated approval procedures for selected drugs in the indications on which we are focusing our efforts. These include accelerated approval under Subpart H of the agency’s NDA approval regulations, fast track drug development procedures, breakthrough drug designation and priority review. At this time, we have not determined whether any of these approval procedures will apply to our current drug candidates.
By leveraging existing preclinical and clinical safety and efficacy data, we seek to build upon an existing knowledge base to accelerate our research. In addition, through our focus on end-stage population which has no current treatment options, regulatory approval for commercialization may sometimes be achieved in an accelerated manner. Accelerated approval by the FDA in this category may be granted on objective response rates and duration of responses rather than demonstration of survival benefit. As a result, studies of drugs to treat end-stage refractory cancer indications have historically involved fewer patients and generally have been faster to complete than studies of drugs for other indications. We are aware that the FDA and other similar agencies are regularly reviewing the use of objective endpoints for commercial approval and that policy changes may impact the size of studies required for approval, timelines and expenditures significantly.
30
The U.S., E.U. and other jurisdictions may grant orphan drug designation to drugs intended to treat a “rare disease or condition,” which, in the U.S., is generally a disease or condition that affects no more than 200,000 individuals. In the E.U., orphan drug designation can be granted if: the disease is life threatening or chronically debilitating and affects no more than 50 in 100,000 persons in the E.U.; without incentive, it is unlikely that the drug would generate sufficient return to justify the necessary investment; and no satisfactory method of treatment for the condition exists or, if it does, the new drug will provide a significant benefit to those affected by the condition. If a product that has an orphan drug designation subsequently receives the first regulatory approval for the indication for which it has such designation, the product is entitled to orphan exclusivity, meaning that the applicable regulatory authority may not approve any other applications to market the same drug for the same indication, except in very limited circumstances, for a period of seven years in the U.S. and 10 years in the E.U. Orphan drug designation does not prevent competitors from developing or marketing different drugs for the same indication or the same drug for different indications. Orphan drug designation must be requested before submitting an NDA or MAA. After orphan drug designation is granted, the identity of the therapeutic agent and its potential orphan use are publicly disclosed. Orphan drug designation does not convey an advantage in, or shorten the duration of, the review and approval process. However, this designation provides an exemption from marketing and authorization fees charged to NDA sponsors under the Prescription Drug Act (PDUFA Fees).
Maintaining substantial compliance with appropriate federal, state and local statutes and regulations requires the expenditure of substantial time and financial resources. Drug manufacturers are required to register their establishments with the FDA and certain state agencies, and after approval, the FDA and these state agencies conduct periodic unannounced inspections to ensure continued compliance with ongoing regulatory requirements, including cGMPs. In addition, after approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval. The FDA may require post-approval testing and surveillance programs to monitor safety and the effectiveness of approved products that have been commercialized. Any drug products manufactured or distributed by us pursuant to FDA approvals are subject to continuing regulation by the FDA, including:
|
|
• |
record-keeping requirements; |
|
|
• |
reporting of adverse experiences with the drug; |
|
|
• |
providing the FDA with updated safety and efficacy information; |
|
|
• |
reporting on advertisements and promotional labeling; |
|
|
• |
drug sampling and distribution requirements; and |
|
|
• |
complying with electronic record and signature requirements. |
In addition, the FDA strictly regulates labeling, advertising, promotion and other types of information on products that are placed on the market. There are numerous regulations and policies that govern various means for disseminating information to health-care professionals as well as consumers, including to industry sponsored scientific and educational activities, information provided to the media and information provided over the Internet. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label.
The FDA has very broad enforcement authority and the failure to comply with applicable regulatory requirements can result in administrative or judicial sanctions being imposed on us or on the manufacturers and distributors of our approved products, including warning letters, refusals of government contracts, clinical holds, civil penalties, injunctions, restitution and disgorgement of profits, recall or seizure of products, total or partial suspension of production or distribution, withdrawal of approvals, refusal to approve pending applications, and criminal prosecution resulting in fines and incarceration. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability. In addition, even after regulatory approval is obtained, later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market.
Sales of our product candidates, if approved, will depend, in part, on the extent to which such products will be covered by third-party payors, such as government health care programs, commercial insurance and managed healthcare organizations. These third-party payors are increasingly limiting coverage or reducing reimbursements for medical products and services. In addition, the U.S. government, state legislatures and foreign governments have continued implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. Third-party payors decide which therapies they will pay for and establish reimbursement levels. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own coverage and reimbursement policies. However, decisions regarding the extent of coverage and amount of reimbursement to be provided for any drug candidates that we develop will be made on a payor-by-payor basis. Each payor determines whether or not it will provide coverage for a therapy, what amount it will pay the manufacturer for the therapy, and on what tier of its formulary it will be placed. The position on a payor’s list of covered drugs, or formulary, generally determines the
31
co-payment that a patient will need to make to obtain the therapy and can strongly influence the adoption of such therapy by patients and physicians. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit our net revenue and results. Decreases in third-party reimbursement for our product candidates or a decision by a third-party payor to not cover our product candidates could reduce physician usage of our product candidates, once approved, and have a material adverse effect on our sales, results of operations and financial condition.
Because of our current and future arrangements with healthcare professionals, principal investigators, consultants, customers and third-party payors, we will also be subject to healthcare regulation and enforcement by the federal government and the states and foreign governments in which we will conduct our business, including our clinical research, proposed sales, marketing and educational programs. Failure to comply with these laws, where applicable, can result in the imposition of significant civil penalties, criminal penalties, or both. The U.S. laws that may affect our ability to operate, among others, include: the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, which governs the conduct of certain electronic healthcare transactions and protects the security and privacy of protected health information; certain state laws governing the privacy and security of health information in certain circumstances, some of which are more stringent than HIPAA and many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts; the federal healthcare programs’ Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual for, or the purchase, order or recommendation of, any good or service for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs; federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent; federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; the Physician Payments Sunshine Act, which requires manufacturers of drugs, devices, biologics, and medical supplies to report annually to the U.S. Department of Health and Human Services information related to payments and other transfers of value to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and ownership and investment interests held by physicians and their immediate family members; and state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers.
In addition, many states have similar laws and regulations, such as anti-kickback and false claims laws that may be broader in scope and may apply regardless of payor, in addition to items and services reimbursed under Medicaid and other state programs. Additionally, to the extent that our product is sold in a foreign country, we may be subject to similar foreign laws.
We are also subject to numerous environmental and safety laws and regulations, including those governing the use and disposal of hazardous materials. The cost of compliance with and any violation of these regulations could have a material adverse effect on our business and results of operations. Although we believe that our safety procedures for handling and disposing of these materials comply with the standards prescribed by state and federal regulations, accidental contamination or injury from these materials may occur. Compliance with laws and regulations relating to the protection of the environment has not had a material effect on our capital expenditures or our competitive position. However, we are not able to predict the extent of government regulation, and the cost and effect thereof on our competitive position, which might result from any legislative or administrative action pertaining to environmental or safety matters.
Competition
The development and commercialization of new drug products is highly competitive. We expect that we will face significant competition from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide with respect to VAL-083 and REM-001 and any other product candidates that we may seek to develop or commercialize in the future. Specifically, due to the large unmet medical need, global demographics and relatively attractive reimbursement dynamics, the oncology market is fiercely competitive and there are a number of large pharmaceutical and biotechnology companies that currently market and sell products or are pursuing the development of product candidates for the treatment of cancer. Our competitors may succeed in developing, acquiring or licensing technologies and drug products that are more effective, have fewer or more tolerable side effects or are less costly than any product candidates that we are currently developing or that we may develop, which could render our product candidates obsolete and noncompetitive.
All of the top ten global pharmaceutical companies and many of the mid-size pharmaceutical companies have a strong research and development and commercial presence in oncology. Smaller companies also focus on oncology, including companies such as ARIAD Pharmaceuticals, Inc., Agios Pharmaceuticals, Inc., BIND Therapeutics, Inc., Clovis Oncology, Inc., Endocyte, Inc., Epizyme, Inc., ImmunoGen, Inc., Incyte Corporation, Infinity Pharmaceuticals, Inc., MacroGenics, Inc., Merrimack Pharmaceuticals, Inc., OncoMed Pharmaceuticals, Inc., Onconova Therapeutics, Inc., Pharmacyclics, Inc., Puma Biotechnology, Inc., Seattle Genetics, Inc. and TESARO, Inc.
32
Several companies are marketing and developing oncology immunotherapy products. Companies with approved marketed oncology products for GBM are Merck (Temodar ®) and Genentech (Avastin ®). Companies with oncology immunotherapy product candidates in clinical development for GBM include, but are not limited to, Northwest Biotherapeutics (DCVax-L), Celldex Therapeutics (Rindopepimut (CDX-110)) and ImmunoCellular Therapeutics (ICT-107).
We are not aware of any therapies specifically approved for CMBC in the US. IGEA Medical S.p.A. is developing an electro-chemotherapy treatment for CMBC. Pinnacle Biologics Inc., a subsidiary of Advanz Pharma Healthcare Corp., sells Photofrin, a first-generation PDT product for treatment of certain endobronchial non-small-cell lung cancers and esophageal cancers. Photofrin is currently in Phase 2 studies in recurrent glioma. To our knowledge, there is no reported development program for Photofrin in CMBC. Rogers Sciences Inc. is a medical device company that is developing a light delivery device for use with PDT treatment of cutaneous cancers that they are currently clinically testing in a Phase 2 study in CMBC patients.
There are numerous therapies currently used to treat CMBC patients including chemotherapy, radiation therapy, surgical excision, hyperthermia, cryotherapy, electro-chemotherapy, topical drugs and intra-lesional chemotherapy injections, but, to our knowledge, there are no PDT therapies currently approved by the FDA for the treatment of CMBC or similar cutaneous cancers. Some topical PDT agents have been approved by the FDA for actinic keratosis which is a precancerous skin condition and they have been approved in some other countries for some conditions that we believe pose low medical risk such as basal cell cancer and acne.
In the BCCNS field we are aware of approved drugs in the U.S., including vismodegib (Eviredge), Odomzo (sonidegib), imiquimod and topical fluorouracil that are sometimes use off-label. PellePharm also recently completed a Phase 3 study in BCCNS but, to our knowledge, has not received marketing approval.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may develop. Our competitors also may obtain FDA or other marketing approval for their products before we are able to obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
Many of our existing and potential future competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical studies, obtaining marketing approvals and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical study sites and patient registration for clinical studies, as well as in acquiring technologies complementary to, or necessary for, our programs.
We expect that our ability to compete effectively will depend upon our ability to:
|
|
• |
successfully and rapidly complete adequate and well-controlled clinical studies that demonstrate statistically significant safety and efficacy and to obtain all requisite regulatory approvals in a cost-effective manner; |
|
|
• |
maintain a proprietary position for our manufacturing processes and other technology; |
|
|
• |
produce our products in accordance with FDA and international regulatory guidelines; |
|
|
• |
attract and retain key personnel; and |
|
|
• |
build or access an adequate sales and marketing infrastructure for any approved products. |
Failure to do one or more of these activities could have an adverse effect on our business, financial condition or results of operations.
Corporate History
We are a Nevada corporation formed on June 24, 2009 under the name Berry Only Inc. On January 25, 2013, we entered into and closed an exchange agreement (the “Exchange Agreement”), with Del Mar Pharmaceuticals (BC) Ltd. (“Del Mar (BC)”), 0959454 B.C. Ltd. (“Callco”), and 0959456 B.C. Ltd. (“Exchangeco”) and the security holders of Del Mar (BC). Upon completion of the Exchange Agreement, Del Mar (BC) became a wholly-owned subsidiary of ours (the “Reverse Acquisition”).
33
On August 19, 2020, we acquired Adgero Biopharmaceuticals Holdings Inc. (“Adgero”) and changed our name from DelMar Pharmaceuticals, Inc. to Kintara Therapeutics, Inc. We are the parent company to the following entities:
|
|
• |
Del Mar (BC), a British Columbia, Canada corporation incorporated on April 6, 2010, which is a clinical stage company with a focus on the development of drugs for the treatment of cancer; |
|
|
• |
Adgero, a Delaware corporation incorporated on October 26, 2015, which is a clinical stage company with a focus on the development of photodynamic therapy for the treatment of rare, unmet medical needs, specifically orphan cancer indications; |
|
|
• |
Adgero Biopharmaceuticals, Inc. a Delaware corporation incorporated on November 16, 2007; and |
|
|
• |
Callco and Exchangeco which are British Columbia, Canada corporations. Callco and Exchangeco were formed to facilitate the Reverse Acquisition. |
On May 8, 2019, we effected a one-for-ten reverse stock split (the “Reverse Stock Split”) of our issued and outstanding and authorized common stock. All per share amounts and number of shares of common stock in this report on Form 10-K reflect the Reverse Stock Split. The Reverse Stock Split does not affect the our authorized preferred stock of 5,000,000 shares; except that, pursuant to the terms of the Certificate of Designations of Series B Convertible Preferred Stock for the issued and outstanding shares of our Series B Convertible Preferred Stock, par value $0.001 per share (the “Series B Preferred Stock”), the conversion price at which shares of Series B Preferred Stock may be converted into shares of common stock will be proportionately adjusted to reflect the Reverse Stock Split.
On June 26, 2019, we amended our articles of incorporation, as amended, to increase the number of authorized shares of common stock from 7,000,000 to 95,000,000 shares.
Research and Development
During the years ended June 30, 2020 and 2019, we recognized $3,630,025 and $3,662,056, respectively, in research and development expenses.
Employees
We have four full-time employees and retain the services of approximately 15 persons on an independent contractor/consultant and contract-employment basis. As such, we currently operate in a “virtual” corporate structure in order to minimize fixed personnel costs.
Available Information
We maintain an internet website at www.kintara.com. We do not incorporate the information on our website into this report and you should not consider it part of this report.
34
An investment in our common stock involves a high degree of risk. In determining whether to purchase our common stock, an investor should carefully consider all of the material risks described below, together with the other information contained in this report before making a decision to purchase our securities. An investor should only purchase our securities if he or she can afford to suffer the loss of his or her entire investment.
Risks Related to Our Business
We are a clinical stage company and have a history of operating losses and expect to incur significant additional operating losses.
We are a clinical stage company with a history of operating losses. For the fiscal years ended June 30, 2020 and 2019, we had net losses of $9.1 million and $8.0 million, respectively and an accumulated deficit of $69.7 million at June 30, 2020. Our prospects must be considered in light of the uncertainties, risks, expenses, and difficulties frequently encountered by companies in similar stages of operations. We expect to incur substantial additional net expenses and losses over the next several years as our research, development, clinical trials, and commercial activities increase.
The amount of future losses and when, if ever, we will achieve profitability are uncertain. Our ability to generate revenue and achieve profitability will depend on, among other things, successful completion of the preclinical and clinical development of our product candidates; obtaining necessary regulatory approvals from the FDA and international regulatory agencies; successful manufacturing, sales and marketing arrangements; and raising sufficient funds to finance our activities. If we are unsuccessful at some or all of these undertakings, our business, prospects and results of operations may be materially adversely affected.
We will need to raise additional capital, which may cause dilution to our stockholders, restrict our operations or require us to relinquish rights to technologies or product candidates.
Until such time, if ever, as we can generate substantial product revenues, we expect to finance our cash needs through a combination of public or private equity offerings, debt financings and/or license and development agreements with collaboration partners. As of June 30, 2020, we had cash and cash equivalents $2,392,402. However, subsequent to June 30, 2020, we completed a private placement in multiple closings for aggregate gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million. We expect the cash available at June 30, 2020 plus the private placement proceeds to fund our planned operations into the fourth quarter of calendar 2021. We will also need to raise additional capital to fund our operations. We do not have any committed external source of funds. To the extent that we raise additional capital through the sale of equity or convertible debt securities, then-existing stockholders’ interests may be materially diluted, and the terms of such securities could include liquidation or other preferences that adversely affect their rights as common stockholders. Debt financing and preferred equity financing, if available, may involve agreements that include restrictive covenants that limit our ability to take specified actions, such as incurring additional debt, making capital expenditures or declaring dividends. In addition, debt financing would result in fixed payment obligations.
If we raise funds through collaborations, strategic partnerships or marketing, distribution or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates or grant licenses on terms that may not be favorable to us. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit, reduce or terminate our product development or future commercialization efforts or grant rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves
Our inability to obtain additional financing could adversely affect our ability to meet our obligations under our planned clinical studies and could negatively impact the timing of our clinical results.
Our ability to meet our obligations and continue the research and development of our product candidates is dependent on our ability to continue to raise adequate financing. We may not be successful in obtaining such additional financing in the amount required at any time, or for any period, or, if available, that it can be obtained on terms satisfactory to us. In the event that we are unable to obtain such additional financing, we may be unable to meet our obligations under our planned clinical studies and we may have to tailor the drug development programs for our drug candidates based on the amount of funding we raise which could negatively impact the timing of our clinical results. In addition, we could be required to cease our operations.
35
We face significant risks related to the COVID-19 pandemic, or the widespread outbreak of any other communicable disease, which could have material and adverse impacts on our business, financial condition, liquidity and results of operations.
We face risks related to health epidemics or outbreaks of communicable diseases, including the recent outbreak around the world of the highly transmissible and pathogenic coronavirus, COVID-19. The outbreak of such communicable diseases could result in a widespread health crisis that could adversely affect general commercial activity and the economies and financial markets of many countries.
In December 2019, a novel strain of coronavirus, COVID-19, was reported to have surfaced in Wuhan, China and on March 11, 2020, was declared a pandemic by the World Health Organization. The ultimate impact of the COVID-19 pandemic on our operations is unknown and will depend on future developments, which are highly uncertain and cannot be predicted with confidence, including the duration of the COVID-19 outbreak, new information which may emerge concerning the severity of the COVID-19 pandemic, and any additional preventative and protective actions that governments, or we, may determine are needed.
To date, many countries around the world have imposed quarantines and restrictions on travel and mass gatherings to slow the spread of COVID-19 and have closed non-essential businesses. As local jurisdictions continue to put restrictions in place, our ability to continue to operate our business may also be limited. Such events may result in a period of business, supply and drug product manufacturing disruption, and in reduced operations, any of which could materially affect our business, financial condition and results of operations.
We are currently conducting clinical studies in multiple countries where there has been a COVID-19 outbreak. Changes in circumstances surrounding COVID-19, such as additional travel limitations imposed by governmental authorities could result in new patients being unable to be enrolled in our studies, or existing patients being unable to continue to receive treatment, could impact the cost of our studies as we may have to enroll additional patients in order to obtain the data necessary to be able to conclude our studies. We cannot predict whether any of our clinical testing sites will withdraw from participation in any of our studies temporarily, or permanently. In addition, even if we are able to fully enroll and treat all patients in our studies, obtaining full data could be impacted by an inability to ship and analyze samples, or otherwise complete data assessment. Further, if the patients enrolled in our clinical studies become infected with COVID-19, we may have more adverse events and deaths in our clinical studies as a result. We may also face difficulties enrolling patients in our clinical studies if the patient populations that are eligible for our clinical studies are impacted by the coronavirus disease. Vulnerable patients, such as the cancer patients enrolled in our clinical studies, may be at a higher risk of contracting COVID-19 and may experience more severe symptoms from the disease, adversely affecting our chances for regulatory approval, or requiring further clinical studies. The continued spread of COVID-19 globally, and the resulting travel restrictions in place by governments to help stop the spread of COVID-19, could adversely impact our clinical study operations, including the ability of our principal investigators and site staff to travel to our clinical study sites, and our ability to recruit and retain principal investigators and site staff who, as healthcare providers, may have heightened exposure to COVID-19 if an outbreak occurs in their geography.
In addition, the continued impact resulting from the COVID-19 outbreak in areas where we have manufacturing operations for our clinical drug supply, or where our suppliers or distributors operate, or if the COVID-19 outbreak in these areas were to increase in severity, and the measures taken by the governments of countries affected, could adversely affect our business, financial condition, or results of operations by limiting our ability to manufacture or ship materials, or by forcing temporary closure of facilities that it relies upon.
The spread of COVID-19, which has caused a broad impact globally, may materially affect us economically. While the potential economic impact brought by, and the duration of, COVID-19 may be difficult to assess or predict, a widespread pandemic could result in significant disruption of global financial markets, reducing our ability to access capital, which could in the future negatively affect our liquidity. In addition, a recession or market correction resulting from the spread of COVID-19 could materially affect our business and the value of our Common Stock.
Integrating our and Adgero’s businesses may be more difficult, time-consuming, or costly than expected.
Kintara and Adgero have operated independently and there can be no assurances that our businesses can be integrated successfully. It is possible that the integration process could result in the loss of key employees, the disruption of either company’s, or both companies’, ongoing businesses or unexpected integration issues, such as higher than expected integration costs and an overall post-completion integration process that takes longer than originally anticipated. Specifically, issues that must be addressed in integrating our operations with Adgero’s in order to realize the anticipated benefits of the Merger so the combined business performs as expected include, among others:
|
|
• |
combining the companies’ separate operational, financial, reporting and corporate functions; |
|
|
• |
integrating the companies’ technologies, products and services; |
|
|
• |
identifying and eliminating redundant and underperforming operations and assets; |
36
|
|
• |
harmonizing the companies’ operating practices, employee development, compensation and benefit programs, internal controls and other policies, procedures and processes; |
|
|
• |
addressing possible differences in corporate cultures and management philosophies; |
|
|
• |
maintaining employee morale and retaining key management and other employees; |
|
|
• |
attracting and recruiting prospective employees; |
|
|
• |
consolidating the companies’ corporate, administrative and information technology infrastructure; |
|
|
• |
coordinating sales, distribution and marketing efforts; |
|
|
• |
managing the movement of certain businesses and positions to different locations; |
|
|
• |
maintaining existing agreements with customers and vendors and avoiding delays in entering into new agreements with prospective customers and vendors; |
|
|
• |
coordinating geographically dispersed organizations; and |
|
|
• |
effecting potential actions that may be required in connection with obtaining regulatory approvals. |
If we are not able to successfully integrate our business with Adgero’s within the anticipated time frame, or at all, the anticipated cost savings, synergies operational efficiencies and other benefits of the Merger may not be realized fully or may take longer to realize than expected, and we may not perform as expected.
While our common stock is expected to be listed on The Nasdaq Capital Market, there is no guarantee as to how long such listing will be maintained.
Our common stock is listed for trading on The Nasdaq Capital Market (“Nasdaq”). We must satisfy Nasdaq’s continued listing requirements, including, among other things, a minimum closing bid price requirement of $1.00 per share for 30 consecutive business days. If a company’s common stock trades for 30 consecutive business days below the $1.00 minimum closing bid price requirement, Nasdaq will send a deficiency notice, advising that such company has been afforded a “compliance period” of 180 calendar days to regain compliance with the applicable requirements. Thereafter, if such a company does not regain compliance with the bid price requirement, a second 180-day compliance period may be available, provided (i) it meets the continued listing requirement for market value of publicly held shares and all other applicable requirements for initial listing on Nasdaq, including stockholder equity requirements, which we may be unable to satisfy (except for the bid price requirement), and (ii) it provides written notice to Nasdaq of its intention to cure this deficiency during the second compliance period by effecting a reverse stock split, if necessary. In the event the company does not regain compliance with Rule 5550(a)(2) prior to the expiration of the initial 180 calendar day period, and if it appears to the Staff of the Listing Qualifications Department of The Nasdaq Stock Market LLC (the “Nasdaq Staff”) that the company will not be able to cure the deficiency, or if the company is not otherwise eligible, the Nasdaq Staff will provide the company with written notification that its securities are subject to delisting from Nasdaq. At that time, the company may appeal the delisting determination to a Hearings Panel.
On September 26, 2019, the Nasdaq Staff notified us that we did not comply with the minimum $1.00 per share bid price requirement for continued listing, as set forth in Nasdaq Listing Rule 5550(a)(2), and we had 180 calendar days, or until March 24, 2020, within which to regain compliance. On March 25, 2020, we received a written notice from the Nasdaq Staff confirming the Company’s eligibility for continued listing of our Common Stock on Nasdaq pursuant to an additional 180 calendar day extension through September 21, 2020. On April 20, 2020, we received a written notice from the Nasdaq Staff stating that, in response to the COVID-19 pandemic and related market conditions, Nasdaq had filed a rule change with the SEC to suspend the compliance period for the minimum closing bid price requirement from April 16, 2020 through June 30, 2020. As a result, we had until December 7, 2020 to regain compliance. To regain compliance, the closing bid price of our Common Stock must be at least $1.00 per share for a minimum of ten consecutive business days or more at the discretion of the Nasdaq Staff.
On August 18, 2020, we received notification from Nasdaq that the closing bid price of our common stock had been at $1.00 per share or greater for ten consecutive business days. Accordingly, we have regained compliance with the minimum bid price requirement.
In the future, if we are unable to maintain compliance with the minimum closing bid price requirement, or if we fail to meet any of the other continued listing requirements, including stockholder equity requirements, our securities may be delisted from Nasdaq and trade on the OTC Markets Group Inc. or other small trading markets, which could reduce the liquidity of our common stock materially and result in a corresponding material reduction in the price of our common stock. In addition, delisting could harm our ability to raise
37
capital through alternative financing sources on terms acceptable to us, or at all, and may result in the potential loss of confidence by investors, employees and business development opportunities. Such a delisting likely would impair your ability to sell or purchase our Common Stock when you wish to do so. Further, if we were to be delisted from Nasdaq, our common stock may no longer be recognized as a “covered security” and we would be subject to regulation in each state in which it offers securities. Thus, delisting from Nasdaq could adversely affect our ability to raise additional financing through the public or private sale of equity securities, would significantly impact the ability of investors to trade our securities and would negatively impact the value and liquidity of our common stock.
The Series C Preferred Stock will have rights, preferences and privileges that will not be held by, and will be preferential to, the rights of holders of our common stock, which could adversely affect the liquidity and financial condition of the Company, and may result in the interests of the holders of Series C Preferred Stock differing from those of the holders of our common stock.
The Series C Preferred Stock will rank on parity with the shares of our Series A Preferred Stock and Series B Preferred Stock with respect to liquidation preferences. Upon any dissolution, liquidation or winding up, whether voluntary or involuntary, holders of Series C Preferred Stock will be entitled to receive distributions out of our assets in an amount per share equal to $1,000 plus all accrued and unpaid dividends, whether capital or surplus before any distributions shall be made on any shares of our common stock.
In addition, holders of Series C Preferred Stock will be entitled to dividends, payable in shares of our common stock at a rate of 10%, 15%, 20% and 25% of the number of shares of common stock issuable upon conversion of the Series C Preferred Stock, on the 12th, 24th, 36th and 48th month, anniversary of the initial closing of the Private Placement, which occurred on August 19, 2020. Dividends will be payable in shares of our common stock and will only be payable to those holders that continue to hold Series C Preferred Stock on the respective anniversary dates of August 19, 2020.
These dividend obligations to the holders of Series C Preferred Stock could limit our ability to obtain additional financing, which could have an adverse effect on our financial condition. The preferential rights described above could also result in divergent interests between the holders of shares of Series C Preferred Stock and the holders of our common stock.
Any issuance of our common stock upon conversion of the Series C Preferred Stock will cause dilution to our then existing stockholders and may depress the market price of our common stock.
The Series C Preferred Stock accrues dividends in shares of our common stock at an initial minimum rate of 10% per annum and following the forty-eight-month anniversary of the initial closing of the Private Placement which occurred on August 19, 2020, such dividend rate could increase to as high as 25% per annum. Each class of Series C Preferred Stock will have a Conversion Price that will be equal to the lesser of (i) the closing price of our common stock on Nasdaq on the date immediately preceding the signing of the applicable binding agreements for the applicable closing date of the Private Placement for which the Series C Preferred Stock is issued or (ii) the average closing price of the our common stock on Nasdaq for the five trading days immediately preceding the signing of the applicable binding agreements for the applicable closing date of the Private Placement for which the Series C Preferred Stock is issued, subject to adjustment. The Conversion Prices for the Series C-1 Preferred Stock, Series C-2 Preferred Stock and Series C-3 Preferred Stock are $1.16, $1.214 and $1.15, respectively.
The issuance of our common stock upon conversion of the Series C Preferred Stock and as payment of dividends on the Series C Preferred Stock will result in immediate and substantial dilution to the interests of holders of our common stock, and such dilution will increase over time in connection with the accrual of dividends on the Series C Preferred Stock.
We may incur future indebtedness that will rank senior to the Series C Preferred Stock or issue additional series of preferred stock that rank on a parity with, or senior to, the Series C Preferred Stock as to dividend payments and liquidation preference.
We may incur substantial amounts of additional debt and other obligations that will rank senior to the Series C Preferred Stock, and the terms of the Series C Preferred Stock do not limit the amount of such debt or other obligations that we may incur. The terms of the Series C Preferred Stock will not prohibit us from issuing additional series of preferred stock that would rank on parity with the Series C Preferred Stock. The Articles allow for the board of directors to create new series of preferred stock without further approval by its stockholders, which could adversely affect the rights of the holders of the Series C Preferred Stock and common stock. The issuances of other series of preferred stock could have the effect of reducing the amounts available to the Series C Preferred Stock in the event of liquidation. If we issue preferred stock with voting rights that dilute the voting power of our common stock, the market price of our common stock could decrease, adversely affecting the value of the Series C Preferred Stock. Additional issuances and sales of preferred stock, or the perception that such issuances and sales could occur, may cause prevailing market prices for our common stock to decline and may adversely affect our ability to raise additional capital in the financial markets at times and prices favorable to it.
38
If we are unable to effectively implement or maintain a system of internal control over financial reporting, we may not be able to accurately or timely report our financial results and our stock price could be adversely affected.
Section 404 of the Sarbanes-Oxley Act of 2002 and related regulations require us to evaluate the effectiveness of our internal control over financial reporting as of the end of each fiscal year, and to include a management report assessing the effectiveness of our internal control over financial reporting in our Annual Report on Form 10-K for that fiscal year. Management determined that as of June 30, 2020 and in past periods, our disclosure controls and procedures and internal control over financial reporting were not effective due to material weaknesses in our internal control over financial reporting related to our limited number of employees in our accounting department and inadequate segregation of duties over authorization, review and recording of transactions, as well as the financial reporting of such transactions. Any failure to implement new or improved controls necessary to remedy the material weaknesses described above, or difficulties encountered in the implementation or operation of these controls, could harm our operations, decrease the reliability of our financial reporting, and cause us to fail to meet our financial reporting obligations, which could adversely affect our business and reduce our stock price.
We are a clinical stage company and may never achieve commercialization of our product candidates or profitability.
We are a clinical stage of development and commercialization of our technologies and product candidates. We have not yet begun to market any products and, accordingly, have not begun or generate revenues from the commercialization of our products. Our products will require significant additional clinical testing and investment prior to commercialization. A commitment of substantial resources by us and, potentially, our partners to conduct time-consuming research and clinical studies will be required if we are to complete the development of our product candidates. There can be no assurance that our product candidates will meet applicable regulatory standards, obtain required regulatory approvals, be capable of being produced in commercial quantities at reasonable costs or be successfully marketed. Our product candidates are not expected to be commercially available for several years, if at all.
We are currently focused on the development of two product candidates.
Our product development efforts are currently focused on two product candidates: VAL-083 for GBM and REM-001 for CMBC. If either VAL-083 or REM-001 fail to achieve clinical endpoints or exhibit unanticipated toxicity or if a superior product is developed by a competitor, our prospects for obtaining regulatory approval and commercialization for either candidate may be negatively impacted. In the long-term, we hope to establish a pipeline of multiple product candidates. However, at this time we do not have any formal agreements granting us any rights to such additional product candidates.
Even if we are able to commercialize any product candidate that we develop, the product may become subject to unfavorable pricing regulations, third-party payor reimbursement practices or healthcare reform initiatives that could harm our business.
The commercial success of our current or future product candidates will depend substantially, both domestically and abroad, on the extent to which the costs of our product candidates will be paid by health maintenance, managed care, pharmacy benefit and similar healthcare management organizations, or reimbursed by government health administration authorities (such as Medicare and Medicaid), private health coverage insurers and other third-party payors. If reimbursement is not available, or is available only to limited levels, we may not be able to successfully commercialize our products. Even if coverage is provided, the approved reimbursement amount may not be high enough to allow us to establish and maintain pricing sufficient to realize a meaningful return on our investment.
There is significant uncertainty related to third-party payor coverage and reimbursement of newly approved drugs. Marketing approvals, pricing and reimbursement for new drug products vary widely from country to country. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing or product licensing approval is granted. In some non-U.S. markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain marketing approval for a product in a particular country, but then be subject to price regulations that delay commercial launch of the product, possibly for lengthy time periods, which may negatively impact the revenues we are able to generate from the sale of the product in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more product candidates, even if our product candidates obtain marketing approval.
Our ability to commercialize VAL-083, REM-001, or any other product candidates will depend in part on the extent to which coverage and reimbursement for these products and related treatments will be available from government health administration authorities, private health insurers and other organizations. Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which medications they will cover and establish reimbursement levels. The healthcare industry is acutely focused on cost containment, both in the United States and elsewhere. Government authorities and third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications, which
39
could affect our ability to sell our product candidates profitably. These payors may not view our products, if any, as cost-effective, and coverage and reimbursement may not be available to our customers, or may not be sufficient to allow our products, if any, to be marketed on a competitive basis. Cost-control initiatives could cause us to decrease the price we might establish for products, which could result in lower than anticipated product revenues. If the prices for our products, if any, decrease or if governmental and other third-party payors do not provide adequate coverage or reimbursement, our prospects for revenue and profitability will suffer.
There may also be delays in obtaining coverage and reimbursement for newly approved drugs, and coverage may be more limited than the indications for which the drug is approved by the FDA or comparable non- U.S. regulatory authorities. Moreover, eligibility for reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Reimbursement rates may vary, by way of example, according to the use of the drug and the clinical setting in which it is used. Reimbursement rates may also be based on reimbursement levels already set for lower cost drugs or may be incorporated into existing payments for other services.
In addition, increasingly, third-party payors are requiring higher levels of evidence of the benefits and clinical outcomes of new technologies and are challenging the prices charged. We cannot be sure that coverage will be available for any product candidate that we, or third-parties, commercialize and, if available, that the reimbursement rates will be adequate. Further, the net reimbursement for drug products may be subject to additional reductions if there are changes to laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the United States. An inability to promptly obtain coverage and adequate payment rates from both government-funded and private payors for any of our product candidates for which we obtain marketing approval could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Pursuant to the terms of our Series B Preferred Stock, the Valent Technologies, LLC (“Valent”) Patent Assignment Agreement, and the St. Cloud Agreement we may be required to pay royalties.
Pursuant to the terms of the Valent Patent Assignment Agreement and our Series B Preferred Stock Certificate of Designation and the related Series B Preferred Royalty Agreement, we will be required to pay royalties if we receive revenue or milestone payments from product sales, or the partnering of VAL-083. If we obtain FDA or EMA approval of VAL-083, and/or if we generate sales of such products, or we receive any proceeds from the licensing or other disposition of VAL-083, we are required to pay to the holders of our Series B Preferred Stock, subject to certain vesting requirements, a low, single-digit royalty. In addition, we are also required to pay a future royalty on all revenues derived from the development and commercialization of VAL-083 to Valent. The royalty payment rights will expire when the patents covering the applicable product expire.
In addition, under our St. Cloud agreement, we must pay to St. Cloud and Steven Rychnovsky, PhD, in the aggregate, a royalty fee of six percent (6%) of net sales during the royalty term on a country-by-country and product-by-product basis with St. Cloud receiving a royalty rate of four and eight tenths percent (4.8%) and Steven Rychnovsky, PhD, receiving a royalty of one and two tenths percent (1.2%). The royalty term for a product commences on the first commercial sale of the product, such as REM-001 Therapy, in any country, and the royalty fee must be paid within 30 days of each calendar quarter during which revenue is collected. The royalty term terminates on the later of (i) the invalidation, revocation, lapse or expiration of the last to expire valid claim on any patent acquired in the St. Cloud Agreement that would be infringed by the sale of the product in the country where the commercial sale takes place or (ii) the expiration of the period for which we hold exclusive marketing rights of the product in the country, if we are granted those rights under the St. Cloud Agreement.
We are dependent on obtaining certain patents and protecting our proprietary rights.
Our success will depend, in part, on our ability to obtain patents, maintain trade secret protection and operate without infringing on the proprietary rights of third parties or having third parties circumvent our rights. We have filed and are actively pursuing patent applications for our products. The patent positions of biotechnology, biopharmaceutical and pharmaceutical companies can be highly uncertain and involve complex legal and factual questions. Thus, there can be no assurance that any of our patent applications will result in the issuance of patents, that we will develop additional proprietary products that are patentable, that any patents issued to us or those that already have been issued will provide us with any competitive advantages or will not be challenged by any third parties, that the patents of others will not impede our ability to do business or that third parties will not be able to circumvent our patents. Furthermore, there can be no assurance that others will not independently develop similar products, duplicate any of our products not under patent protection, or, if patents are issued to us, design around the patented products we developed or will develop.
We may be required to obtain licenses from third parties to avoid infringing patents or other proprietary rights. No assurance can be given that any licenses required under any such patents or proprietary rights would be made available, if at all, on terms we find acceptable. If we do not obtain such licenses, we could encounter delays in the introduction of products or could find that the development, manufacture or sale of products requiring such licenses could be prohibited.
40
A number of pharmaceutical, biopharmaceutical and biotechnology companies and research and academic institutions have developed technologies, filed patent applications or received patents on various technologies that may be related to or affect our business. Some of these technologies, applications or patents may conflict with our technologies or patent applications. Such conflict could limit the scope of the patents, if any, that we may be able to obtain or result in the denial of our patent applications. In addition, if patents that cover our activities are issued to other companies, there can be no assurance that we would be able to obtain licenses to these patents at a reasonable cost or be able to develop or obtain alternative technology. If we do not obtain such licenses, we could encounter delays in the introduction of products, or could find that the development, manufacture or sale of products requiring such licenses could be prohibited. In addition, we could incur substantial costs in defending ourselves in suits brought against us on patents it might infringe or in filing suits against others to have such patents declared invalid.
Patent applications in the U.S. are maintained in secrecy and not published if either: (i) the application is a provisional application or (ii) the application is filed and we request no publication, and certify that the invention disclosed “has not and will not” be the subject of a published foreign application. Otherwise, U.S. applications or foreign counterparts, if any, publish 18 months after the priority application has been filed. Since publication of discoveries in the scientific or patent literature often lag behind actual discoveries, we cannot be certain that we or any licensor were the first creator of inventions covered by pending patent applications or that we or such licensor was the first to file patent applications for such inventions. Moreover, we might have to participate in interference proceedings declared by the U.S. Patent and Trademark Office (the “USPTO”) to determine priority of invention, which could result in substantial cost to us, even if the eventual outcome were favorable to us. There can be no assurance that our patents, if issued, would be held valid or enforceable by a court or that a competitor’s technology or product would be found to infringe such patents.
Moreover, we may be subject to third-party preissuance submissions of prior art to the USPTO, or become involved in opposition, derivation, reexamination, inter partes review, post-grant review or interference proceedings challenging our patent rights or the patent rights of others. An adverse determination in any such submission, proceeding or litigation could reduce the scope of, or invalidate, our patent rights, allow third parties to commercialize our technology or products and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights.
Even if our patent applications issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors from competing with us, or otherwise provide us with any competitive advantage. Our competitors may be able to circumvent our patents by developing similar or alternative technologies or products in a non-infringing manner.
The issuance of a patent is not conclusive as to its inventorship, scope, validity or enforceability, and our patents may be challenged in courts or patent offices in the United States and abroad. Such challenges may result in loss of exclusivity or freedom to operate, or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
In addition, the protection of intellectual property rights in China (where one of our clinical product candidates, VAL-083, is manufactured pursuant to a collaboration agreement with the only manufacturer presently licensed by the CFDA to manufacture VAL-083 for the China market, and where VAL-083 is approved for the treatment of CML and lung cancer) is relatively weak compared to the United States, which may negatively affect our ability to generate royalty revenue from sales of VAL-083 in China.
Much of our know-how and technology may not be patentable. To protect our rights, we require employees, consultants, advisors and collaborators to enter into confidentiality agreements. There can be no assurance, however, that these agreements will provide meaningful protection for our trade secrets, know-how or other proprietary information in the event of any unauthorized use or disclosure. Further, our business may be adversely affected by competitors who independently develop competing technologies, especially if we obtain no, or only narrow, patent protection.
We do not hold any patents covering our laser light source or light delivery device for REM-001.
Our laser light source and light delivery device are not currently covered by any patents; We do not have any patents pending, and do not currently intend to seek patent protection for these devices. As a result, competitors may be able to offer and sell products or drug delivery technology, as the case may be, using the same technology as our laser light source and/or light delivery devices, so long as these competitors do not infringe any other valid patents that it or third-parties hold.
41
While we plan to protect our proprietary information related to our laser light source and light delivery device as trade secrets through certain agreements with our employees, consultants, agents and other organizations to which we have disclosed our proprietary information, we cannot give any assurance that these agreements will provide effective protection for our proprietary information in the event of unauthorized use or disclosure of such information. If other laser light sources or light delivery devices are approved and marketed, we will be unable to prevent them from competing with REM-001 Therapy in the marketplace using a different drug molecule that is not encompassed by any of our owned or licensed patents. We expect that the presence of one or more competing products would reduce our market share and could negatively impact price levels and third-party reimbursement policies for REM-001 Therapy, any of which would materially affect our business.
We may be unable to protect our patents and proprietary rights.
Our future success will depend to a significant extent on our ability to:
|
|
• |
obtain and keep patent protection for our products and technologies on an international basis; |
|
|
• |
enforce our patents to prevent others from using our inventions; |
|
|
• |
maintain and prevent others from using our trade secrets; and |
|
|
• |
operate and commercialize products without infringing on the patents or proprietary rights of others. |
We can provide no assurance that our patent rights will afford any competitive advantages and these rights may be challenged or circumvented by third parties. Further, patents may not be issued on any of our pending patent applications in the U.S. or abroad. Because of the extensive time required for development, testing and regulatory review of a product candidate, it is possible that before a product candidate can be commercialized, any related patent may expire, or remain in existence for only a short period following commercialization, reducing or eliminating any advantage of the patent.
If we sue others for infringing on our patents, a court may determine that such patents are invalid or unenforceable. Even if the validity of our patent rights is upheld by a court, a court may not prevent the alleged infringement of our patent rights on the grounds that such activity is not covered by our patent claims.
In addition, third parties may sue us for infringing on their patents. In the event of a successful claim of infringement against us, we may be required to:
|
|
• |
defend litigation or administrative proceedings; |
|
|
• |
pay substantial damages; |
|
|
• |
stop using our technologies and methods; |
|
|
• |
stop certain research and development efforts; |
|
|
• |
develop non-infringing products or methods; and |
|
|
• |
obtain one or more licenses from third parties. |
If required, we can provide no assurance that we will be able to obtain such licenses on acceptable terms, or at all. If we are sued for infringement, we could encounter substantial delays in development, manufacture and commercialization of our product candidates. Any litigation, whether to enforce our patent rights or to defend against allegations that we infringed third-party rights, will be costly, time consuming, and may distract management from other important tasks.
As is commonplace in the biotechnology and pharmaceutical industry, we employ individuals who were previously employed at other biotechnology or pharmaceutical companies, including our competitors or potential competitors. To the extent our employees are involved in research areas which are similar to those areas in which they were involved at their former employers, we may be subject to claims that such employees and/or we have inadvertently or otherwise used or disclosed the alleged trade secrets or other proprietary information of the former employers. Litigation may be necessary to defend against such claims, which could result in substantial costs and be a distraction to management and which may have a material adverse effect on us, even if we are successful in defending such claims.
42
We are subject to various government regulations.
The manufacture and sale of human therapeutic and diagnostic products in the U.S., Canada and foreign jurisdictions are governed by a variety of statutes and regulations. These laws require approval of manufacturing facilities, controlled research and testing of products and government review and approval of a submission containing manufacturing, preclinical and clinical data in order to obtain marketing approval based on establishing the safety and efficacy of the product for each use sought, including adherence to current cGMP during production and storage, and control of marketing activities, including advertising and labeling.
VAL-083, REM-001 and any other products we may develop will require significant development, preclinical and clinical testing and investment of substantial funds prior to its commercialization. The process of obtaining required approvals can be costly and time-consuming, and there can be no assurance that we will successfully develop any future products that will prove to be safe and effective in clinical studies or receive applicable regulatory approvals. Markets other than the U.S. and Canada have similar restrictions. Potential investors and shareholders should be aware of the risks, problems, delays, expenses and difficulties which we may encounter in view of the extensive regulatory environment which controls our business.
We may request priority review for our product candidates in the future. The FDA may not grant priority review for our product candidates. Moreover, even if the FDA designated such product for priority review, that designation may not lead to a faster regulatory review or approval process and, in any event, would not assure FDA approval.
We may be eligible for priority review designation for our product candidates if the FDA determines such product candidate offers major advances in treatment or provides a treatment where no adequate therapy exists. A priority review designation means that the goal for the FDA to review an application is six months, rather than the standard review period of ten months. The FDA has broad discretion with respect to whether or not to grant priority review status to a product candidate, so even if we believe a particular product candidate is eligible for such designation or status, the FDA may decide not to grant it. Thus, while the FDA has granted priority review to other oncology disease products, our product candidates, should we determine to seek priority review, may not receive similar designation. Moreover, even if our product candidate is designated for priority review, such a designation does not necessarily mean a faster regulatory review process or necessarily confer any advantage with respect to approval compared to conventional FDA procedures. Receiving priority review from the FDA does not guarantee approval within an accelerated timeline or thereafter.
We believe we may in some instances be able to secure approval from the FDA or comparable non-U.S. regulatory authorities to use accelerated development pathways. If we are unable to obtain such approval, we may be required to conduct additional preclinical studies or clinical studies beyond those that it contemplates, which could increase the expense of obtaining, and delay the receipt of, necessary marketing approvals.
We anticipate that we may seek an accelerated approval pathway for our product candidates. Under the accelerated approval provisions in the Federal Food, Drug, and Cosmetic Act (“FDCA”), and the FDA’s implementing regulations, the FDA may grant accelerated approval to a product designed to treat a serious or life-threatening condition that provides meaningful therapeutic benefit over available therapies upon a determination that the product has an effect on a surrogate endpoint or intermediate clinical endpoint that is reasonably likely to predict clinical benefit. The FDA considers a clinical benefit to be a positive therapeutic effect that is clinically meaningful in the context of a given disease, such as irreversible morbidity or mortality. For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign, or other measure that is thought to predict clinical benefit, but is not itself a measure of clinical benefit. An intermediate clinical endpoint is a clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit. The accelerated approval pathway may be used in cases in which the advantage of a new drug over available therapy may not be a direct therapeutic advantage, but is a clinically important improvement from a patient and public health perspective. If granted, accelerated approval is usually contingent on the sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the drug’s clinical benefit. If such post-approval studies fail to confirm the drug’s clinical benefit, the FDA may withdraw its approval of the drug.
Prior to seeking such accelerated approval, we will seek feedback from the FDA and will otherwise evaluate our ability to seek and receive such accelerated approval. There can also be no assurance that after our evaluation of the feedback and other factors we will decide to pursue or submit a New Drug Application (“NDA”), for accelerated approval or any other form of expedited development, review or approval. Similarly, there can be no assurance that after subsequent FDA feedback that we will continue to pursue or apply for accelerated approval or any other form of expedited development, review or approval, even if we initially decide to do so. Furthermore, if we decide to submit an application for accelerated approval or under another expedited regulatory designation (e.g., breakthrough therapy designation), there can be no assurance that such submission or application will be accepted or that any expedited development, review or approval will be granted on a timely basis, or at all. The FDA or other non-U.S. authorities could also require us to conduct further studies prior to considering our application or granting approval of any type. A failure to
43
obtain accelerated approval or any other form of expedited development, review or approval for any of our product candidates that we decide to seek accelerated approval for would result in a longer time period to commercialization of such product candidate, could increase the cost of development of such product candidate and could harm our competitive position in the marketplace.
We have conducted, and may in the future conduct, clinical studies for certain of our product candidates at sites outside the United States, and the FDA may not accept data from studies conducted in such locations.
We have conducted and may in the future choose to conduct one or more of our clinical studies outside the United States. Although the FDA may accept data from clinical studies conducted outside the United States, acceptance of this data is subject to certain conditions imposed by the FDA. For example, the clinical study must be well designed and conducted and performed by qualified investigators in accordance with ethical principles. The study population must also adequately represent the U.S. population, and the data must be applicable to the U.S. population and U.S. medical practice in ways that the FDA deems clinically meaningful. Generally, the patient population for any clinical studies conducted outside of the United States must be representative of the population for whom we intend to seek approval in the United States. In addition, while these clinical studies are subject to the applicable local laws, FDA acceptance of the data will be dependent upon its determination that the studies also complied with all applicable U.S. laws and regulations. There can be no assurance that the FDA will accept data from studies conducted outside of the United States. If the FDA does not accept the data from any of our clinical studies that we determine to conduct outside the United States, it would likely result in the need for additional studies, which would be costly and time-consuming and delay or permanently halt our development of the product candidate.
In addition, the conduct of clinical studies outside the United States could have a significant impact on us. The risks inherent in conducting international clinical studies include:
|
|
• |
foreign regulatory requirements that could restrict or limit our ability to conduct our clinical studies; |
|
|
• |
administrative burdens of conducting clinical studies under multiple foreign regulatory schema; |
|
|
• |
foreign exchange fluctuations; and |
|
|
• |
diminished protection of intellectual property in some countries. |
If our clinical studies fail to demonstrate safety and efficacy to the satisfaction of the FDA and comparable non-U.S. regulators, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our product candidates.
We are not permitted to commercialize, market, promote or sell any product candidate in the United States without obtaining marketing approval from the FDA. Comparable non-U.S. regulatory authorities, such as the EMA, impose similar restrictions. We may never receive such approvals. We must complete extensive preclinical development and clinical studies to demonstrate the safety and efficacy of our product candidates in humans before we will be able to obtain these approvals.
Clinical testing is expensive, difficult to design and implement, can take many years to complete and is inherently uncertain as to outcome. We have not previously submitted an NDA to the FDA or similar drug approval filings to comparable non-U.S. regulatory authorities for any product candidate.
Any inability to successfully complete preclinical and clinical development could result in additional costs to us and impair our ability to generate revenues from product sales, regulatory and commercialization milestones and royalties. In addition, if (1) we are required to conduct additional clinical studies or other testing of our product candidates beyond the studies and testing that we contemplate, (2) we are unable to successfully complete clinical studies of our product candidates or other testing, (3) the results of these studies or tests are unfavorable, uncertain or are only modestly favorable, or (4) there are unacceptable safety concerns associated with our product candidate, we, in addition to incurring additional costs, may:
|
|
• |
be delayed in obtaining marketing approval for our product candidates; |
|
|
• |
not obtain marketing approval at all; |
|
|
• |
obtain approval for indications or patient populations that are not as broad as we intended or desired; |
|
|
• |
obtain approval with labeling that includes significant use or distribution restrictions or significant safety warnings, including boxed warnings; |
|
|
• |
be subject to additional post-marketing testing or other requirements; or |
|
|
• |
be required to remove the product from the market after obtaining marketing approval. |
44
If we experience any of a number of possible unforeseen events in connection with clinical studies of our product candidates, potential marketing approval or commercialization of our product candidates could be delayed or prevented.
We may experience numerous unforeseen events during, or as a result of, clinical studies that could delay or prevent marketing approval of our product candidates, including:
|
|
• |
clinical studies of our product candidates may produce unfavorable or inconclusive results; |
|
|
• |
we may decide, or regulators may require us, to conduct additional clinical studies or abandon product development programs; |
|
|
• |
the number of patients required for clinical studies of our product candidates may be larger than we anticipate, patient enrollment in these clinical studies may be slower than we anticipate or participants may drop out of these clinical studies at a higher rate than we anticipate; |
|
|
• |
data safety monitoring committees may recommend suspension, termination or a clinical hold for various reasons, including concerns about patient safety; |
|
|
• |
regulators or IRBs may suspend or terminate the study or impose a clinical hold for various reasons, including noncompliance with regulatory requirements or concerns about patient safety; |
|
|
• |
patients with serious, life-threatening diseases included in our clinical studies may die or suffer other adverse medical events for reasons that may not be related to our product candidates; |
|
|
• |
participating patients may be subject to unacceptable health risks; |
|
|
• |
patients may not complete clinical studies due to safety issues, side effects, or other reasons; |
|
|
• |
changes in regulatory requirements and guidance may occur, which require us to amend clinical study protocols to reflect these changes; |
|
|
• |
our third-party contractors, including those manufacturing our product candidates or components or ingredients thereof or conducting clinical studies on our behalf, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner or at all; |
|
|
• |
regulators or institutional review boards, or IRBs may not authorize us or our investigators to commence a clinical study or conduct a clinical study at a prospective study site; |
|
|
• |
we may experience delays in reaching or fail to reach agreement on acceptable clinical study contracts or clinical study protocols with prospective study sites; |
|
|
• |
patients who enroll in a clinical study may misrepresent their eligibility to do so or may otherwise not comply with the clinical study protocol, resulting in the need to drop the patients from the clinical study, increase the needed enrollment size for the clinical study or extend the clinical study’s duration; |
|
|
• |
we may have to suspend or terminate clinical studies of our product candidates for various reasons, including a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of a product candidate; |
|
|
• |
regulators or IRBs may require that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or their respective standards of conduct, a finding that the participants are being exposed to unacceptable health risks, undesirable side effects or other unexpected characteristics of the product candidate or findings of undesirable effects caused by a chemically or mechanistically similar drug or drug candidate; |
|
|
• |
the FDA or comparable non-U.S. regulatory authorities may fail to approve or subsequently find fault with the manufacturing processes or facilities of third-party manufacturers with which we enter into agreements for clinical and commercial supplies; |
|
|
• |
the FDA or comparable non-U.S. regulatory authorities may disagree with our clinical study design or our interpretation of data from preclinical studies and clinical studies; |
|
|
• |
the supply or quality of raw materials or manufactured product candidate or other materials necessary to conduct clinical studies of our product candidates may be insufficient, inadequate, delayed, or not available at an acceptable cost, or we may experience interruptions in supply; and |
|
|
• |
the approval policies or regulations of the FDA or comparable non-U.S. regulatory authorities may significantly change in a manner rendering our clinical data insufficient to obtain marketing approval. |
45
Product development costs for us will increase if we experience delays in testing or pursuing marketing approvals and we may be required to obtain additional funds to complete clinical studies and prepare for possible commercialization of our product candidates. We do not know whether any preclinical tests or clinical studies will begin as planned, will need to be restructured or will be completed on schedule, or at all. Significant preclinical or clinical study delays also could shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before we do and impair our ability to successfully commercialize our product candidates and may harm our business and results of operations. In addition, many of the factors that cause, or lead to, clinical study delays may ultimately lead to the denial of marketing approval of our product candidates.
If we experience delays or difficulties in the enrollment of patients in clinical studies, our product candidates may not achieve clinical development on our anticipated timeline, or at all, and our receipt of necessary regulatory approvals could be delayed or prevented.
We may not be able to initiate or continue clinical studies for VAL-083, REM-001 or any other product candidate if we are unable to locate and enroll a sufficient number of eligible patients to participate in clinical studies. Patient enrollment is a significant factor in the timing of clinical studies, and is affected by many factors, including:
|
|
• |
the size and nature of the patient population; |
|
|
• |
the severity of the disease under investigation; |
|
|
• |
the proximity of patients to clinical sites; |
|
|
• |
the eligibility criteria for the study; |
|
|
• |
the design of the clinical study; |
|
|
• |
efforts to facilitate timely enrollment; |
|
|
• |
competing clinical studies; and |
|
|
• |
clinicians’ and patients’ perceptions as to the potential advantages and risks of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. |
Our inability to enroll a sufficient number of patients for our clinical studies could result in significant delays or may require us to abandon one or more clinical studies altogether. Enrollment delays in our clinical studies may result in increased development costs for our product candidates, delay or halt the development of and approval processes for our product candidates and jeopardize our ability to achieve our clinical development timeline and goals, including the dates by which we will commence, complete and receive results from clinical studies. Enrollment delays may also delay or jeopardize our ability to commence sales and generate revenues from our product candidates. Any of the foregoing could cause our value to decline and limit our ability to obtain additional financing, if needed.
Positive results in previous clinical studies of VAL-083 and REM-001may not be replicated in future clinical studies, which could result in development delays or a failure to obtain marketing approval.
Positive results in previous clinical studies of VAL-083 and REM-001 may not be predictive of similar results in future clinical studies. Also, interim results during a clinical study do not necessarily predict final results. A number of companies in the pharmaceutical and biotechnology industries have suffered significant setbacks in late-stage clinical studies even after achieving promising results in early-stage development. Accordingly, the results from the completed preclinical studies and clinical studies for VAL-083 and REM-001 may not be predictive of the results we may obtain in later stage studies. Our clinical studies may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical studies. Moreover, clinical data are often susceptible to varying interpretations and analyses, and many companies that believed their product candidates performed satisfactorily in preclinical studies and clinical studies have nonetheless failed to obtain FDA or EMA, or other regulatory agency, approval for their products.
FDA approval of VAL-083, REM-001, or future product candidates may be denied.
There can be no assurance that the FDA will ultimately approve our NDAs. The FDA may deny approval of VAL-083 or REM-001 for many reasons, including:
|
|
• |
we may be unable to demonstrate to the satisfaction of the FDA that our products are safe and effective for its intended uses; |
|
|
• |
the FDA may disagree with our interpretation of data from the clinical studies; |
46
|
|
• |
we may be unable to demonstrate that any clinical or other benefits of our products outweigh any safety or other perceived risks; or |
|
|
• |
we may not be able to successfully address any other issues raised by the FDA. |
If VAL-083 or REM-001 fail to receive FDA approval, our business and prospects will be materially adversely impacted.
We expect to rely on orphan drug status to develop and commercialize our product candidates, but our orphan drug designations may not confer marketing exclusivity or other expected commercial benefits as anticipated.
Market exclusivity afforded by orphan drug designation is generally offered as an incentive to drug developers to invest in developing and commercializing products for unique diseases that impact a limited number of patients. The FDA may grant orphan drug designation to drugs intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States. Qualification to maintain orphan drug status is generally monitored by the regulatory authorities during the orphan drug exclusivity period, currently seven years from the date of approval in the United States.
For VAL-083, we have been granted orphan drug designation in the United States for GBM, ovarian cancer, and medulloblastoma, and in Europe for GBM. In addition, for REM-001 the FDA granted our request that tin ethyl etiopurpurin (the active pharmaceutical ingredient in REM-001) be designated as an orphan drug for treatment of BCCNS. We also hold an orphan drug designation that was initially awarded to Miravant for tin ethyl etiopurpurin for the prevention of access graft disease in hemodialysis patients.
We expect to rely on orphan drug exclusivity for our product candidates. It is possible that the incidence and prevalence numbers for GBM, CMBC, and access graft disease could change. Should the incidence and prevalence of these diseases materially increase, it is possible that the orphan drug designation, and related market exclusivity, in the United States could be lost. Further, while we have been granted these orphan designations, the FDA can still approve different drugs for use in treating the same indication or disease, which would create a more competitive market for us and our revenues, if any, will be diminished.
Further, it is possible that another company also holding orphan drug designation for the same product candidate will receive marketing approval for the same indication before we do. If that were to happen, our applications for that indication may not be approved until the competing company’s period of exclusivity expires. Even if we are the first to obtain marketing authorization for an orphan drug indication, there are circumstances under which a competing product may be approved for the same indication during the seven-year period of marketing exclusivity, such as if the later product is shown to be clinically superior to the orphan product, or if the later product is deemed a different product than ours. Further, the seven-year marketing exclusivity would not prevent competitors from obtaining approval of the same product candidate as ours for indications other than those in which we have been granted orphan drug designation, or for the use of other types of products in the same indications as our orphan products.
If the market opportunities for our product candidates are smaller than we believe they are, our future revenues may be adversely affected and our business may suffer. Because the target patient populations of our product candidates are small, we must be able to successfully identify patients and capture a significant market share to achieve and maintain profitability.
We focus our research and product development on treatments for orphan cancer indications. Our projections of both the number of people who have failed other therapies or have limited medical options, are based on estimates. These estimates may prove to be incorrect and new studies may change the estimated incidence or prevalence. The number of patients in the United States, Europe and elsewhere may turn out to be lower than expected or may not be otherwise amenable to treatment with our products, or new patients may become increasingly difficult to identify or gain access to, all of which would adversely affect our results of operations and our business. Additionally, because our target patient populations are small, we will be required to capture a significant market share to achieve and maintain profitability.
We may be required to suspend or discontinue clinical studies due to unexpected side effects or other safety risks that could preclude approval of our products.
Our clinical studies may be suspended at any time for a number of reasons. For example, we may voluntarily suspend or terminate our clinical studies if at any time we believe that they present an unacceptable risk to the clinical study patients. In addition, the FDA or other regulatory agencies may order the temporary or permanent discontinuation of our clinical studies at any time if they believe that the clinical studies are not being conducted in accordance with applicable regulatory requirements or that they present an unacceptable safety risk to the clinical study patients.
47
Administering any product candidate to humans may produce undesirable side effects. These side effects could interrupt, delay or halt clinical studies of our product candidates and could result in the FDA or other regulatory authorities denying further development or approval of our product candidates for any or all targeted indications. Ultimately, some or all of our product candidates may prove to be unsafe for human use. Moreover, we could be subject to significant liability if any volunteer or patient suffers, or appears to suffer, adverse health effects or even death as a result of participating in our clinical studies.
Our product candidates may cause undesirable adverse events or have other properties that could delay or prevent their regulatory approval, limit the commercial profile of an approved label, and/or result in significant negative consequences following regulatory approval, if any, including withdrawal from the market.
The REM-001 Therapy may exhibit undesirable and unintended side effects that may prevent or limit its commercial adoption and use. Even upon receiving approval by the FDA and other regulatory authorities, our products may later exhibit adverse side effects that prevent widespread use or necessitate withdrawal from the market. The manifestation of such side effects could cause its business to suffer.
Undesirable adverse events caused by our product candidates could cause us or regulatory authorities to interrupt, delay or halt clinical trials and may result in a more restrictive label, a delay or denial of regulatory approval by the FDA or other comparable regulatory authorities, or a significant change in our clinical protocol or even our development plan. For example, in the four clinical trials of REM-001 therapy conducted by Miravant, there were a total of 17 serious adverse events, a large portion of which were related to necrosis of treated lesions. One adverse event that has been seen with REM-001 Therapy is a period of photosensitivity after receiving REM-001 Therapy. This period of photosensitivity is generally dose dependent and typically declines over time. A second such adverse event is pain that arises or results from the treatment. Treatment-related pain has been experienced by some patients and it is often treated with analgesics but in some cases more aggressive treatment can be required.
If clinical trials of our product candidates reveal a high and unacceptable severity or prevalence of certain adverse events, our trials could be suspended or terminated and the FDA and/or other comparable regulatory authorities could order us to cease further development of, or deny approval of, our product candidates for any or all targeted indications. Adverse events related to our candidates also may affect patient recruitment or the ability of enrolled subjects to complete the trial and could result in potential liability claims. Any of these occurrences may significantly harm our reputation, business, financial condition and prospects.
Additionally, adverse events associated with our future approved products candidates may lead to potentially significant negative consequences, which include, but are not limited to, the following:
|
|
• |
suspension of our marketing of the product; |
|
|
• |
withdrawal or revocation by regulatory authorities of their approvals of or the licenses for the product; |
|
|
• |
the requirement by regulatory authorities to conduct additional post-approval clinical trials, add additional warnings to, or otherwise change, the label of the product, or create a medication guide outlining the risks of such side effects for distribution to patients; |
|
|
• |
restrictions on the distribution of the product or imposition of burdensome implementation requirements on us through the establishment of a Risk Evaluation and Mitigation Strategy (“REMS”) or similar strategy as may be required by the FDA or a comparable regulatory authority; |
|
|
• |
changes in the way the product is distributed or administered; |
|
|
• |
regulatory investigations, government enforcement actions or litigation proceedings, and being held liable for harm caused to subjects or patients; |
|
|
• |
removal of products from the marketplace; and |
|
|
• |
harm to our reputation. |
Any of these events could prevent us from achieving or maintaining market acceptance of any particular product candidate that is approved and could significantly harm our business, results of operations and prospects.
Our plan to achieve marketing approval of REM-001 Therapy depends partly on the accuracy of its preliminary efficacy analysis of REM-001 Therapy CMBC trial data. While we believe the results of our preliminary efficacy analysis accurately reflect the actual clinical trial results, a detailed analysis overseen by regulatory experts may yield different results.
48
We plan to utilize existing REM-001 Therapy clinical trial data as supportive data when seeking marketing approval of REM-001 Therapy for the treatment of CMBC. Between February 1996 and January 1999, Miravant, with support from certain corporate partners, conducted four clinical trials for the treatment of CMBC using REM-001 Therapy. As part of our review of REM-001 Therapy’s data package, we noted that while Miravant’s investigators had done a safety analysis of all treated patients, these reports indicated an efficacy analysis was only performed on two of their four clinical trials. Notably, there had been no efficacy analysis on the other two trials which constituted approximately half of the CMBC patients who were treated with REM-001 Therapy. We originally performed a preliminary efficacy analysis on the data from all four CMBC trials, including the two that had not previously been analyzed. We then engaged regulatory experts who were either former FDA employees with directly related experience in reviewing similar oncology treatments who were then acting as independent consultants or individuals who have provided senior regulatory guidance to major pharmaceutical or medical device companies in situations that led to regulatory approval. These individuals guided us in conducting a second more in-depth analysis that yielded results consistent with our original analysis. Following that, we compiled a briefing document and submitted questions to FDA. While we believe the results of our preliminary efficacy analysis, and subsequent analysis conducted under the guidance of these experts which was consistent with its original preliminary analysis, accurately reflect the actual clinical trial results and that the age of the underlying data from the clinical studies is not material, a more in-depth review may yield different conclusions. Such differing results may negatively impact our ability to pursue or achieve, or result in delays to obtain, marketing approval of REM-001 Therapy. There can be no certainty that results from our analyses done to date or results from future analyses that we may undertake will be sufficiently complete to satisfy FDA requests or that any results will be favorable to us.
Our REM-001 Therapy clinical trial data may not be deemed acceptable by the FDA to support our new drug applications.
In seeking regulatory approval for REM-001, we intend to rely at least in part upon data gathered by Miravant Medical Technologies in its initial Phase 1 studies and in four later Phase 2/3 clinical studies that were conducted approximately 20 years ago. Based on our initial interactions with the FDA, we believe the agency will accept these results as supportive data but we cannot ultimately be certain that the FDA will accept data that old to support our new drug applications. Also based on our initial interactions with the FDA, we believe our plans for manufacturing investigational test materials will lead to investigational test materials that FDA will recognize as being sufficiently comparable to Miravant’s materials and also suitable for further investigational trials but FDA may later raise questions about the similarity of Miravant’s investigational testing material versus its manufactured investigational testing material, or may raise questions about the processes and methods under which this old data was collected or may raise additional concerns regarding the elapsed time period. If the FDA does not accept this data, we will have to incur significant costs which may require additional capital to redo some or all of the Miravant studies or supplement these studies with additional studies.
We may not receive regulatory approvals for our product candidates or there may be a delay in obtaining such approvals.
Our products and our ongoing development activities are subject to regulation by regulatory authorities in the countries in which we or our collaborators and distributors wish to test, manufacture or market our products. For instance, the FDA will regulate the product in the U.S. and equivalent authorities, such as the EMA, will regulate in Europe. Regulatory approval by these authorities will be subject to the evaluation of data relating to the quality, efficacy and safety of the product for its proposed use, and there can be no assurance that the regulatory authorities will find our data sufficient to support product approval of VAL-083 or any future product candidates.
The time required to obtain regulatory approval varies between countries. The FDA is required to facilitate the development and expedite the review of drugs and biologics that are intended for the treatment of a serious or life-threatening disease or condition and which demonstrate the potential to address unmet medical needs for the condition. Filling an unmet medical need is defined as providing a therapy where none exists or providing a therapy that may be potentially better than available therapy. Under the fast track program, the sponsor of a new drug or biologic candidate may request the FDA to designate the product for a specific indication as a fast track product concurrent with or after the filing of the IND for the product candidate. The FDA must determine if the product candidate qualifies for fast track designation within 60 days after receipt of the sponsor’s request. In the U.S., for products without “Fast Track” status, it can take over eighteen (18) months after submission of an application for product approval to receive the FDA’s decision. Even with Fast Track status, FDA review and decision can take over twelve (12) months.
In December 2017, the FDA granted Fast Track designation for VAL-083 in patients with rGBM.
49
Different regulators may impose their own requirements and may refuse to grant, or may require additional data before granting, an approval, notwithstanding that regulatory approval may have been granted by other regulators. Regulatory approval may be delayed, limited or denied for a number of reasons, including insufficient clinical data, the product not meeting safety or efficacy requirements or any relevant manufacturing processes or facilities not meeting applicable requirements as well as case load at the regulatory agency at the time.
We may fail to comply with regulatory requirements.
Our success will be dependent upon our ability, and our collaborative partners’ abilities, to maintain compliance with regulatory requirements, including cGMP, and safety reporting obligations. The failure to comply with applicable regulatory requirements can result in, among other things, fines, injunctions, civil penalties, total or partial suspension of regulatory approvals, refusal to approve pending applications, recalls or seizures of products, operating and production restrictions and criminal prosecutions.
Even if one of our product candidates receives marketing approval, it may fail to achieve the degree of market acceptance by physicians, patients, third-party payors and others in the medical community necessary for commercial success and the market opportunity for the product candidate may be smaller than our estimates.
We have never commercialized a product. Even if VAL-083, REM-001, or any other product candidates is approved by the appropriate regulatory authorities for marketing and sale, it may nonetheless fail to gain sufficient market acceptance by physicians, patients, third-party payors and others in the medical community. For example, physicians are often reluctant to switch their patients from existing therapies even when new and potentially more effective or convenient treatments enter the market. Further, patients often acclimate to the therapy that they are currently taking and do not want to switch unless their physicians recommend switching products or they are required to switch therapies due to lack of reimbursement for existing therapies.
Efforts to educate the medical community and third-party payors on the benefits of our product candidates may require significant resources and may not be successful. If our product candidates are approved but do not achieve an adequate level of market acceptance, we may not generate significant revenues and we may not become profitable. The degree of market acceptance of VAL-083, REM-001, or any other product candidate, if approved for commercial sale, will depend on a number of factors, including:
|
|
• |
the efficacy and safety of the product; |
|
|
• |
the potential advantages of the product compared to alternative treatments; |
|
|
• |
the prevalence and severity of any side effects; |
|
|
• |
the clinical indications for which the product is approved; |
|
|
• |
whether the product is designated under physician treatment guidelines as a first-line therapy or as a second- or third-line therapy; |
|
|
• |
limitations or warnings, including distribution or use restrictions, contained in the product’s approved labeling; |
|
|
• |
our ability to offer the product for sale at competitive prices; |
|
|
• |
our ability to establish and maintain pricing sufficient to realize a meaningful return on our investment; |
|
|
• |
the product’s convenience and ease of administration compared to alternative treatments; |
|
|
• |
the willingness of the target patient population to try, and of physicians to prescribe, the product; |
|
|
• |
the strength of sales, marketing and distribution support; |
|
|
• |
the approval of other new products for the same indications; |
|
|
• |
changes in the standard of care for the targeted indications for the product; |
|
|
• |
the timing of market introduction of our approved products as well as competitive products and other therapies; |
|
|
• |
availability and amount of reimbursement from government payors, managed care plans and other third-party payors; |
|
|
• |
adverse publicity about the product or favorable publicity about competitive products; and |
|
|
• |
potential product liability claims. |
The potential market opportunities for our product candidates are difficult to estimate precisely. Our estimates of the potential market opportunities are predicated on many assumptions, including industry knowledge and publications, third-party research reports and other surveys. While we believe that our internal assumptions are reasonable, these assumptions involve the exercise of significant
50
judgment on the part of our management, are inherently uncertain and the reasonableness of these assumptions has not been assessed by an independent source. If any of the assumptions proves to be inaccurate, the actual markets for our product candidate could be smaller than our estimates of the potential market opportunities.
If one of our product candidates receives marketing approval and we, or others, later discover that the drug is less effective than previously believed or causes undesirable side effects that were not previously identified, our ability to market the drug could be compromised.
Clinical studies of our product candidates are conducted in carefully defined subsets of patients who have agreed to enter into clinical studies. Consequently, it is possible that our clinical studies may indicate an apparent positive effect of a product candidate that is greater than the actual positive effect, if any, or alternatively fail to identify undesirable side effects. If, following approval of one of our product candidates, we, or others, discover that the drug is less effective than previously believed or causes undesirable side effects that were not previously identified, any of the following adverse events could occur:
|
|
• |
regulatory authorities may withdraw their approval of the drug or seize the drug; |
|
|
• |
we may be required to recall the drug or change the way the drug is administered; |
|
|
• |
additional restrictions may be imposed on the marketing of, or the manufacturing processes for, the particular drug; |
|
|
• |
we may be subject to fines, injunctions or the imposition of civil or criminal penalties; |
|
|
• |
regulatory authorities may require the addition of labeling statements, such as a “black box” warning or a contraindication; |
|
|
• |
we may be required to create a Medication Guide outlining the risks of the previously unidentified side effects for distribution to patients; |
|
|
• |
we could be sued and held liable for harm caused to patients; |
|
|
• |
the drug may become less competitive; and |
|
|
• |
our reputation may suffer. |
Any of these events could have a material and adverse effect on our operations and business and could adversely impact our stock price.
Any product candidate for which we obtain marketing approval, along with the manufacturing processes, qualification testing, post-approval clinical data, labeling and promotional activities for such product, will be subject to continual and additional requirements of the FDA and other regulatory authorities.
These requirements include submissions of safety and other post-marketing information, reports, registration and listing requirements, good manufacturing practices, or GMP requirements relating to quality control, quality assurance and corresponding maintenance of records and documents, and recordkeeping. Even if marketing approval of any of our product candidates is granted, the approval may be subject to limitations on the indicated uses for which the product may be marketed or to conditions of approval, or contain requirements for costly post-marketing testing and surveillance to monitor the safety or efficacy of the product. The FDA closely regulates the post-approval marketing and promotion of pharmaceutical products to ensure such products are marketed only for the approved indications and in accordance with the provisions of the approved labeling.
In addition, later discovery of previously unknown problems with our products, manufacturing processes, or failure to comply with regulatory requirements, may lead to various adverse results, including:
|
|
• |
restrictions on such products, manufacturers or manufacturing processes; |
|
|
• |
restrictions on the labeling or marketing of a product; |
|
|
• |
restrictions on product distribution or use; |
|
|
• |
requirements to conduct post-marketing clinical studies; |
|
|
• |
requirements to institute a risk evaluation mitigation strategy, or REMS, to monitor safety of the product post-approval; |
|
|
• |
warning letters issued by the FDA or other regulatory authorities; |
51
|
|
• |
withdrawal of the products from the market; |
|
|
• |
refusal to approve pending applications or supplements to approved applications that we submit; |
|
|
• |
recall of products, fines, restitution or disgorgement of profits or revenue; |
|
|
• |
suspension, revocation or withdrawal of marketing approvals; |
|
|
• |
refusal to permit the import or export of our products; and |
|
|
• |
injunctions or the imposition of civil or criminal penalties. |
If we are unable to establish sales, marketing and distribution capabilities or enter into acceptable sales, marketing and distribution arrangements with third parties, we may not be successful in commercializing any product candidates that we develop, if and when those product candidates are approved.
We do not have a sales, marketing or distribution infrastructure and have limited experience in the sale, marketing or distribution of pharmaceutical products. To achieve commercial success for any approved product, we must either develop a sales and marketing organization, outsource these functions to third parties, or license our product candidates to others. If approved, we may seek to license VAL-083 or REM-001 to a large pharmaceutical company with greater resources and experience than us. We may not be able to license VAL-083 or REM-001 on reasonable terms, if at all. The development of sales, marketing and distribution capabilities will require substantial resources, will be time-consuming and could delay any product launch. We expect that we will commence the development of these capabilities prior to receiving approval of our product candidates. If the commercial launch of a product candidate for which we recruit a sales force and establish marketing and distribution capabilities is delayed or does not occur for any reason, we could have prematurely or unnecessarily incurred these commercialization costs. Such a delay may be costly, and our investment could be lost if we cannot retain or reposition our sales and marketing personnel. In addition, we may not be able to hire or retain a sales force in the United States that is sufficient in size or has adequate expertise in the medical markets that we plan to target. If we are unable to establish or retain a sales force and marketing and distribution capabilities, our operating results may be adversely affected. If a potential partner has development or commercialization expertise that we believe is particularly relevant to our product candidates, then we may seek to collaborate with that potential partner even if we believe we could otherwise develop and commercialize the product independently.
We expect to seek one or more strategic partners for commercialization of our product candidates outside the United States. As a result of entering into arrangements with third parties to perform sales, marketing and distribution services, our product revenues or the profitability of these product revenues may be lower, perhaps substantially lower, than if we were to directly market and sell products in those markets. Furthermore, we may be unsuccessful in entering into the necessary arrangements with third parties or may be unable to do so on terms that are favorable to us. In addition, we may have little or no control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our products effectively.
If we do not establish sales and marketing capabilities, either on our own or in collaboration with third parties, we will not be successful in commercializing our product candidates.
We face substantial competition from other pharmaceutical and biotechnology companies and our operating results may suffer if we fail to compete effectively.
The development and commercialization of new drug products is highly competitive. We expect that we will face significant competition from major pharmaceutical companies, specialty pharmaceutical companies and biotechnology companies worldwide with respect to VAL-083, REM-001, and any other product candidates that we may seek to develop or commercialize in the future. Specifically, due to the large unmet medical need, global demographics and relatively attractive reimbursement dynamics, the oncology market is fiercely competitive and there are a number of large pharmaceutical and biotechnology companies that currently market and sell products or are pursuing the development of product candidates for the treatment of cancer. Our competitors may succeed in developing, acquiring or licensing technologies and drug products that are more effective, have fewer or more tolerable side effects or are less costly than any product candidates that we are currently developing or that we may develop, which could render our product candidates obsolete and noncompetitive. All of the top ten global pharmaceutical companies and many of the mid-size pharmaceutical companies have a strong research and development and commercial presence in oncology. Several companies are marketing and developing oncology immunotherapy products.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may develop. Our competitors also may obtain FDA or other marketing approval for their products before we are able to obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
52
Many of our existing and potential future competitors have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical studies, obtaining marketing approvals and marketing approved products than our does. Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These competitors also compete with us in recruiting and retaining qualified scientific and management personnel and establishing clinical study sites and patient registration for clinical studies, as well as in acquiring technologies complementary to, or necessary for, our programs.
If we are unable to obtain, or are delayed in obtaining, state regulatory licenses for the distribution of our products, we would not be able to sell our product candidates.
The majority of states require manufacturer and/or wholesaler licenses for the sale and distribution of drugs into that state. The application process is complicated, time consuming and requires dedicated personnel or a third-party to oversee and manage. If we are delayed in obtaining these state licenses, or denied the licenses, even with FDA approval, we would not be able to sell or ship product into that state which would adversely affect our sales and revenues.
We rely on key personnel and members of management and, if we are unable to retain or motivate key personnel or management, or hire qualified personnel, we may not be able to grow effectively.
We are dependent on certain members of our management, scientific and drug development staff and consultants, the loss of services of one or more of whom could materially adversely affect us.
We currently have four full-time employees, and retain the services of approximately 15 persons on an independent contractor/consultant and contract-employment basis. Our ability to manage growth effectively will require us to continue to implement and improve our management systems and to recruit and train new employees. Although we have done so in the past and expect to do so in the future, there can be no assurance that we will be able to successfully attract and retain skilled and experienced personnel.
Our success depends in large part upon our ability to attract and retain highly qualified personnel. We compete in our hiring efforts with other pharmaceutical and biotechnology companies, as well as universities and nonprofit research organizations, and we may have to pay higher salaries to attract and retain personnel, which would be very costly.
We may be subject to foreign exchange fluctuation.
Our functional and reporting currency is the United States dollar. We maintain bank accounts in United States and Canadian dollars. A portion of our expenditures are in foreign currencies, most notably in Canadian dollars, and therefore we are subject to foreign currency fluctuations, which may, from time to time, impact our financial position and results. We may enter into hedging arrangements under specific circumstances, typically through the use of forward or futures currency contracts, to minimize the impact of increases in the value of the Canadian dollar. In order to minimize our exposure to foreign exchange fluctuations we may hold sufficient Canadian dollars to cover our expected Canadian dollar expenditures.
Product liability lawsuits against us could divert our resources, cause us to incur substantial liabilities and limit commercialization of any products that we may develop.
We face an inherent risk of product liability claims as a result of the clinical testing of our product candidates despite obtaining appropriate informed consents from our clinical study participants. We will face an even greater risk if we commercially sell any product that we may develop. For example, we may be sued if any product we develop allegedly causes injury or is found to be otherwise unsuitable during clinical testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability or a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our product candidates. Regardless of the merits or eventual outcome, liability claims may result in:
|
|
• |
decreased demand for our product candidates or products that we may develop; |
|
|
• |
injury to our reputation and significant negative media attention; |
|
|
• |
withdrawal of clinical study participants; |
|
|
• |
significant costs to defend resulting litigation; |
53
|
|
• |
substantial monetary awards to study participants or patients; |
|
|
• |
loss of revenue; |
|
|
• |
reduced resources of our management to pursue our business strategy; and |
|
|
• |
the inability to commercialize any products that we may develop. |
Although we maintain general liability insurance, this insurance may not fully cover potential liabilities that we may incur. The cost of any product liability litigation or other proceeding, even if resolved in our favor, could be substantial. We will need to increase our insurance coverage if and when we begin selling any product candidate that receives marketing approval. In addition, insurance coverage is becoming increasingly expensive. If we are unable to obtain or maintain sufficient insurance coverage at an acceptable cost or to otherwise protect against potential product liability claims, it could prevent or inhibit the development and commercial production and sale of our product candidates, which could adversely affect our business, financial condition, results of operations and prospects.
Risks Related to Our Dependence on Third Parties
We rely on third parties to conduct clinical studies for our product candidate. Any failure by a third-party to meet our obligations with respect to the clinical development of our product candidate may delay or impair our ability to obtain regulatory approval for our product candidate.
We rely on academic institutions and private oncology centers to conduct our clinical studies. Our reliance on third parties to conduct clinical studies could, depending on the actions of such third parties, jeopardize the validity of the clinical data generated and adversely affect our ability to obtain marketing approval from the FDA or other applicable regulatory authorities.
Such clinical study arrangements provide us with information rights with respect to the clinical data, including access to and the ability to use and reference the data, including for our own regulatory filings, resulting from the clinical studies. If investigators or institutions breach their obligations with respect to the clinical studies of our product candidate, or if the data proves to be inadequate, then our ability to design and conduct any future clinical studies may be adversely affected.
We rely, and expect to continue to rely, on third parties to conduct our clinical studies, and those third parties may not perform satisfactorily, including failing to meet deadlines for the completion of such studies.
We currently rely on third-party clinical research organizations, or CROs, to conduct our clinical studies. We expect to continue to rely on third parties, such as CROs, clinical data management organizations, medical institutions and clinical investigators, to conduct our clinical studies. Our agreements with these third parties generally allow the third-party to terminate the agreement at any time. If we are required to enter into alternative arrangements because of any such termination the introduction of our product candidates to market could be delayed.
Our reliance on these third parties for research and development activities will reduce our control over these activities but will not relieve us of our responsibilities. For example, we design our clinical studies and will remain responsible for ensuring that each of our clinical studies are conducted in accordance with the general investigational plan and protocols for the study. Moreover, the FDA requires us to comply with standards, commonly referred to as good clinical practices, or GCPs, for conducting, recording and reporting the results of clinical studies to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of study participants are protected. Our reliance on third parties that we do not control does not relieve us of these responsibilities and requirements. We also are required to register ongoing clinical studies and post the results of completed clinical studies on a government-sponsored database, Clinicaltrials.gov, within specified timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
Furthermore, these third parties may also have relationships with other entities, some of which may be our competitors. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our clinical studies in accordance with regulatory requirements or our stated protocols, we will not be able to obtain, or may be delayed in obtaining, marketing approvals for our product candidates and will not be able to, or may be delayed in our efforts to, successfully commercialize our product candidates.
We also expect to rely on other third parties to store and distribute drug supplies for our clinical studies. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidate or commercialization of our products, producing additional losses and depriving us of potential product revenue.
54
We may seek to enter into collaborations with third parties for the development and commercialization of our product candidate. If we fail to enter into such collaborations, or such collaborations are not successful, we may not be able to capitalize on the market potential of our product candidate.
We may seek third-party collaborators for development and commercialization of our product candidate. Our likely collaborators for any marketing, distribution, development, licensing or broader collaboration arrangements include large and mid-size pharmaceutical companies, regional and national pharmaceutical companies, non-profit organizations, government agencies, and biotechnology companies. We are currently party to a limited number of such arrangements and have limited control over the amount and timing of resources that our collaborators dedicate to the development or commercialization of our product candidate. Our ability to generate revenues from these arrangements will depend on our collaborators’ abilities to successfully perform the functions assigned to them in these arrangements.
Collaborations involving our product candidate currently pose, and will continue to pose, the following risks to us:
|
|
• |
collaborators have significant discretion in determining the efforts and resources that they will apply to these collaborations; |
|
|
• |
collaborators may not pursue development and commercialization of our product candidate or may elect not to continue or renew development or commercialization programs based on preclinical or clinical study results, changes in the collaborators’ strategic focus or available funding, or external factors such as an acquisition that diverts resources or creates competing priorities; |
|
|
• |
collaborators may delay clinical studies, provide insufficient funding for a clinical study program, stop a clinical study or abandon a product candidate, repeat or conduct new clinical studies or require a new formulation of a product candidate for clinical testing; |
|
|
• |
collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our product candidate if the collaborators believe that competitive products are more likely to be successfully developed or can be commercialized under terms that are more economically attractive than ours; |
|
|
• |
collaborators with marketing and distribution rights to one or more products may not commit sufficient resources to the marketing and distribution of such product or products; |
|
|
• |
collaborators may not properly maintain or defend our intellectual property rights or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our intellectual property or proprietary information or expose us to potential litigation; |
|
|
• |
collaborators may infringe the intellectual property rights of third parties, which may expose us to litigation and potential liability; |
|
|
• |
disputes may arise between the collaborators and us that result in the delay or termination of the research, development or commercialization of our product candidate or that result in costly litigation or arbitration that diverts management attention and resources; and |
|
|
• |
collaborations may be terminated and, if terminated, may result in a need for additional capital to pursue further development or commercialization of the applicable product candidates. |
Collaboration agreements may not lead to development or commercialization of our product candidate in the most efficient manner or at all. If a collaborator of ours were to be involved in a business combination, the continued pursuit and emphasis on our product development or commercialization program could be delayed, diminished or terminated.
If we are not able to establish collaborations, we may have to alter our development and commercialization plans.
Our drug development programs and the potential commercialization of our product candidate will require substantial additional cash to fund expenses. We may decide to collaborate with pharmaceutical and biotechnology companies for the development and potential commercialization of our product candidate.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration and the proposed collaborator’s evaluation of a number of factors. Those factors may include the design or results of preclinical studies or clinical studies, the likelihood of approval by the FDA or similar regulatory authorities outside the United States, the potential market for the subject product candidate, the costs and complexities of manufacturing and delivering such product candidate to patients, the potential of competing products, the existence of uncertainty with respect to our ownership of technology, which can exist if there is a challenge to such ownership without regard to the merits of the challenge and
55
industry and market conditions generally. The collaborator may also consider alternative product candidates or technologies for similar indications that may be available to collaborate on and whether such a collaboration could be more attractive than the one with us for our product candidate. We may also be restricted under future license agreements from entering into agreements on certain terms with potential collaborators. Collaborations are complex and time-consuming to negotiate and document. In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators.
We may not be able to negotiate collaborations on a timely basis, on acceptable terms, or at all. If we are unable to do so, we may have to curtail the development of our product candidates, reduce or delay our development program, delay our potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms or at all. If we do not have sufficient funds, we may not be able to further develop our product candidate or bring it to market and generate product revenue.
We currently manufacture VAL-083 at a single location. Any disruption at this facility could adversely affect our business and results of operations.
We have engaged a single manufacturer to produce VAL-083 GMP active pharmaceutical ingredient and a single manufacturer to produce VAL-083 drug product for our clinical studies. In addition, we have relied on our manufacturing partner, Guangxi Wuzhou Pharmaceutical Company, for the manufacture of clinical supply of VAL-083 for our preclinical and Phase 2 clinical studies being conducted in China. If our manufacturer’s facility were damaged or destroyed, or otherwise subject to disruption, it would require substantial lead-time to replace our clinical supply. In such event, we would be forced to rely entirely on other third-party contract manufacturers for an indefinite period of time. We do not currently have established relationships with any back-up manufacturers. At this time no drug product has been manufactured by a third-party back-up manufacturer. Any disruptions or delays by our third-party manufacturers or Guangxi Wuzhou Pharmaceutical Company or their failure to meet regulatory compliance could impair our ability to develop VAL-083, which would adversely affect our business and results of operations.
We rely on these third-party manufacturers to provide drug product supply for all of our clinical studies for VAL-083. There is no assurance that such a supplier will be able to meet our needs from a technical, timing, or cost-effective manner. Our failure to enter into appropriate agreements with such a third-party manufacturer would delay, or halt, our clinical studies.
We do not have a clinical supply of REM-001. Moreover, we do not have our own manufacturing facilities nor have we contracted with third-parties to manufacture product for us. If we are unable to contract with suitable third-party manufacturers, or if third-party manufacturers fail to meet applicable regulatory requirements or to supply us for any reason, we will be unable to complete clinical studies for REM-001 Therapy and our business will be materially impaired.
We do not have a clinical supply of REM-001. Our plan calls for the use of a third-party manufacturer to produce the product for us. If and when approved, we intend to have a third-party manufacture commercial supplies of the product as well. We have not yet completed the transfer of the technology or manufactured the product at these facilities and our failure to timely do so will delay the commencement of our clinical studies and may also impact the timing for the submission of our NDA for REM-001 Therapy.
We do not have a clinical supply of light delivery devices for use with REM-001 Therapy. Moreover, we do not have our own manufacturing facilities nor have we contracted a third-party to manufacture these devices for us. If we are unable to contract a third-party manufacturer, or if a third-party manufacturer fails to meet applicable regulatory requirements or to supply us for any reason, we will be unable to complete clinical studies for REM-001 Therapy and our business will be materially impaired.
We do not have a clinical supply of REM-001 Therapy light delivery devices. Our plan calls for the use of a third-party manufacturer to produce these devices for us. We have not yet contracted a third-party manufacturer and our failure to timely do so will delay the commencement of our clinical studies and the submission of our NDA for REM-001 Therapy.
56
We are planning to use laser light devices that the FDA finds to be functionally equivalent to the Miravant devices in our planned clinical studies. We do not have our own manufacturing facilities for conducting these activities nor have we contracted a third-party to manufacture these devices for us. If we are unable to contract a third-party manufacturer, or if a third-party manufacturer fails to meet applicable regulatory requirements or to supply it for any reason, we will be unable to complete clinical studies for REM-001 Therapy and our business will be materially impaired.
Our plan relies on using laser light devices that the FDA finds to be functionally equivalent to the Miravant devices. Our plan calls for the use of a third-party manufacturer to produce new laser devices for us. We have not yet contracted such a third-party and our failure to timely do so will delay the commencement of our clinical studies and the submission of our NDA for REM-001 Therapy.
We may become subject to liabilities related to risks inherent in working with hazardous materials.
Our discovery and development processes involve the controlled use of hazardous and radioactive materials. We are subject to federal, provincial and local laws and regulations governing the use, manufacture, storage, handling and disposal of such materials and certain waste products. Although we believe that our safety procedures for handling and disposing of such materials comply with the standards prescribed by such laws and regulations, the risk of accidental contamination or injury from these materials cannot be completely eliminated. In the event of such an accident, we could be held liable for any damages that result and any such liability could exceed our resources. We are not specifically insured with respect to this liability. Although we believe that we are in compliance in all material respects with applicable environmental laws and regulations and currently do not expect to make material capital expenditures for environmental control facilities in the near-term, there can be no assurance that we will not be required to incur significant costs to comply with environmental laws and regulations in the future, or that our operations, business or assets will not be materially adversely affected by current or future environmental laws or regulations.
Risks Related to Our Common Stock
The market price of our common stock is, and is likely to continue to be, highly volatile and subject to wide fluctuations.
The market price of our common stock is highly volatile and could be subject to wide fluctuations in response to a number of factors that are beyond our control, including:
|
|
• |
variations in our quarterly operating results; |
|
|
• |
announcements that our revenue or income are below analysts’ expectations; |
|
|
• |
general economic slowdowns; |
|
|
• |
sales of large blocks of our common stock; and |
|
|
• |
announcements by us or our competitors of significant contracts, acquisitions, strategic partnerships, joint ventures or capital commitments. |
Our Articles allow for our board of directors to create new series of preferred stock without further approval by our stockholders, which could adversely affect the rights of the holders of our Common Stock.
Our board of directors has the authority to fix and determine the relative rights and preferences of preferred stock. Our board of directors has the authority to issue up to 5,000,000 shares of our preferred stock (of which 278,530 shares have been designated Series A Preferred Stock and are issued and outstanding, and 1,000,000 shares have been designated as Series B Preferred Stock, of which 648,613 shares are issued and outstanding, as of June 30, 2020) without further stockholder approval. In addition, 28,400 have been designated as Series C (22,000 as Series C-1, 2,700 as Series C-2, and 3,700 as Series C-3) of which 25,028 are outstanding. As a result, our board of directors could authorize the issuance of additional series of preferred stock that would grant to holders the preferred right to our assets upon liquidation, the right to receive dividend payments before dividends are distributed to the holders of common stock and the right to the redemption of the shares, together with a premium, prior to the redemption of our Common Stock. In addition, our board of directors could authorize the issuance of a series of preferred stock that has greater voting power than our Common Stock or that is convertible into our Common Stock, which could decrease the relative voting power of our Common Stock or result in dilution to our existing stockholders. Although we have no present intention to issue any additional shares of preferred stock or to create any additional series of preferred stock, we may issue such shares in the future.
57
Issuance of our Common Stock upon exercise of warrants or options, or conversion of Series B or Preferred C Preferred Stock may depress the price of our Common Stock.
As of September 15, 2020, we had 23,543,892 shares of common stock issued and outstanding, outstanding, warrants to purchase 12,446,779 shares of common stock, warrants to purchase 2,504 Series C Preferred Stock that upon conversion are convertible into 2,152,667 shares of common stock, outstanding stock options to purchase 6,243,872 shares of common stock, 648,613 outstanding shares of Series B Preferred Stock that are convertible into 162,177 shares of common stock, 25,028 outstanding shares of Series C Preferred Stock that are convertible into 21,516,484 shares of common stock. All warrants and stock options are convertible, or exercisable into, one share of common stock. Each Series B convertible preferred share is convertible into 0.25 shares of common stock and the Series C convertible Preferred Stock (issued in three series) are convertible into a total of 21,516,484 shares of common stock.
The issuance of shares of our common stock upon the exercise of outstanding warrants or options, or the conversion of our Series B, or Series C-1, C-2, and C-3 Series Preferred Stock, could result in substantial dilution to our stockholders, which may have a negative effect on the price of our common stock.
We do not intend to pay cash dividends on our common stock for the foreseeable future.
We have paid no cash dividends on our common stock to date and we do not anticipate paying any dividends to holders of our common stock in the foreseeable future. While our future dividend policy will be based on the operating results and capital needs of the business, we currently anticipate that any earnings will be retained to finance our future expansion and for the implementation of our business plan. Investors should take note of the fact that a lack of a dividend can further affect the market value of our common stock, and could significantly affect the value of any investment in us.
58
FORWARD-LOOKING STATEMENTS
This annual report on Form 10-K contains forward-looking statements made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 under Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. Forward-looking statements include statements with respect to our beliefs, plans, objectives, goals, expectations, anticipations, assumptions, estimates, intentions and future performance, and involve known and unknown risks, uncertainties and other factors, which may be beyond our control, and which may cause our actual results, performance or achievements to be materially different from future results, performance or achievements expressed or implied by such forward-looking statements. All statements other than statements of historical fact are statements that could be forward-looking statements. You can identify these forward-looking statements through our use of words such as “may,” “can,” “anticipate,” “assume,” “should,” “indicate,” “would,” “believe,” “contemplate,” “expect,” “seek,” “estimate,” “continue,” “plan,” “point to,” “project,” “predict,” “could,” “intend,” “target,” “potential” and other similar words and expressions of the future.
There are a number of important factors that could cause the actual results to differ materially from those expressed in any forward-looking statement made by us. These factors include, but are not limited to:
|
|
• |
our ability to raise funds for general corporate purposes and operations, including our research activities and clinical studies; |
|
|
• |
the impact of the recent outbreak of COVID-19 on our business and operations or on the economy generally; |
|
|
• |
our ability to recruit qualified management and technical personnel; |
|
|
• |
the cost, timing, scope and results of our clinical studies; |
|
|
• |
our ability to expand our international business; |
|
|
• |
our ability to obtain and maintain required regulatory approvals for our products; |
|
|
• |
our expectations regarding the use of our existing cash; |
|
|
• |
our ability to realize the anticipated benefits from the acquisition of Adgero; |
|
|
• |
our ability to obtain or maintain patents or other appropriate protection for the intellectual property utilized in our current and planned products; |
|
|
• |
our ability to develop and commercialize products without infringing the intellectual property rights of third parties; and |
|
|
• |
the other factors discussed in the “Risk Factors” section and elsewhere in this Annual Report. |
The foregoing does not represent an exhaustive list of matters that may be covered by the forward-looking statements contained herein or risk factors that we are faced with that may cause our actual results to differ from those anticipated in our forward-looking statements. Please see “Risk factors” in this Annual Report on Form 10-K under Part I, Item 1A, for additional risks which could adversely impact our business and financial performance.
All forward-looking statements are expressly qualified in their entirety by this cautionary notice. You are cautioned not to place undue reliance on any forward-looking statements, which speak only as of the date of this report or the date of the document incorporated by reference into this report. We have no obligation, and expressly disclaim any obligation, to update, revise or correct any of the forward-looking statements, whether as a result of new information, future events or otherwise. We have expressed our expectations, beliefs and projections in good faith and we believe they have a reasonable basis. However, we cannot assure you that our expectations, beliefs or projections will result or be achieved or accomplished.
Item 1B. Unresolved Staff Comments.
Not required for a smaller reporting company.
Our corporate headquarters are currently located at 12707 High Bluff Drive, Suite 200, San Diego CA, 92130. The current rent at that location under a one-year renewable lease is $189 per month. We also rent our administrative offices located at Suite 720-999 West Broadway, Vancouver, British Columbia, Canada on a month-to-month basis at a rate of $3,187 (CA$4,357) per month. During the year ended June 30, 2020, we recorded a total of $40,130 as rent expense (2019 - $52,926).
59
In addition, Valent, which is owned by Dr. Dennis Brown, our Chief Scientific Officer, leases facilities in California and we have access to such facilities pursuant to an informal unwritten arrangement with Valent. Our leased premises, academic relationships, and access to the Valent facility are sufficient to meet the immediate needs of our business, research and operations.
There are no legal proceedings to which we are a party or any of our property is the subject.
Item 4. Mine Safety Disclosures.
Not applicable.
60
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Since August 20, 2020, our common stock has been listed on The Nasdaq Capital Market under the symbol “KTRA”. From July 12, 2016 until August 19, 2020 our common stock was listed on The Nasdaq Capital Market under the symbol “DMPI”. Previously, our common stock was quoted on the OTC.QX, and prior to that, on the OTCQB.
As of September 15, 2020, there were approximately 477 holders of record of our common stock.
Dividends
We have never declared or paid any cash dividends on our common stock. We currently intend to retain future earnings, if any, to finance the expansion of our business. As a result, we do not anticipate paying any cash dividends in the foreseeable future.
Sales of Unregistered Securities
During the three months ended June 30, 2020, we issued 3,700 shares of common stock as dividends on our outstanding shares of Series B Preferred Stock, 2,096 shares of common stock in relation to services received by us, and 5,000 common shares upon the conversion of remaining Exchangeco shares.
In connection with the foregoing, we relied upon the exemption from registration provided by Section 4(a)(2) of the Securities Act of 1933, as amended, for transactions not involving a public offering.
Issuer Purchases of Equity Securities
None.
Item 6. Selected Financial Data.
Not required for a smaller reporting company.
61
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION
AND RESULTS OF OPERATIONS
This Management’s Discussion and Analysis (“MD&A”) contains “forward-looking statements”, within the meaning of the Private Securities Litigation Reform Act of 1995, which represent our projections, estimates, expectations, or beliefs concerning, among other things, financial items that relate to management’s future plans or objectives or to our future economic and financial performance. In some cases, you can identify these statements by terminology such as “may”, “should”, “plans”, “believe”, “will”, “anticipate”, “estimate”, “expect” “project”, or “intend”, including their opposites or similar phrases or expressions. You should be aware that these statements are projections or estimates as to future events and are subject to a number of factors that may tend to influence the accuracy of the statements. These forward-looking statements should not be regarded as a representation by us or any other person that our events or plans will be achieved. You should not unduly rely on these forward-looking statements, which speak only as of the date of this report. Except as may be required under applicable securities laws, we undertake no obligation to publicly revise any forward-looking statement to reflect circumstances or events after the date of this report or to reflect the occurrence of unanticipated events.
You should review the factors and risks we describe under “Risk Factors” in this report on Form 10-K for the year ended June 30, 2020 and in our other filings with the Securities and Exchange Commission, available at www.sec.gov. Actual results may differ materially from any forward-looking statement.
Kintara Therapeutics, Inc. is the parent company of Del Mar (BC), a British Columbia, Canada corporation, and Adgero Biopharmaceuticals Holdings, Inc., a Delaware corporation (“Adgero”), which are clinical stage companies with a focus on the development of drugs for the treatment of cancer. The Company is also the parent company to Callco and Exchangeco which are British Columbia, Canada corporations. Callco and Exchangeco were formed to facilitate the Reverse Acquisition. In connection with the merger described below, the Company is also the parent company of Adgero Biopharmaceuticals, Inc., formerly a wholly-owned subsidiary of Adgero.
References to “we”, “us”, and “our”, refer to Kintara Therapeutics, Inc. and our wholly-owned subsidiaries, Del Mar (BC), Adgero, Adgero Biopharmaceuticals, Inc., Callco and Exchangeco.
Corporate History
We are a Nevada corporation formed on June 24, 2009 under the name Berry Only, Inc. On January 25, 2013, we entered into and closed an exchange agreement (the “Exchange Agreement”), with Del Mar Pharmaceuticals (BC) Ltd. (“Del Mar (BC)”), 0959454 B.C. Ltd. (“Callco”), and 0959456 B.C. Ltd. (“Exchangeco”) and the security holders of Del Mar (BC). Upon completion of the Exchange Agreement, Del Mar (BC) became our wholly-owned subsidiary (the “Reverse Acquisition”).
On June 10, 2020, we entered into an Agreement and Plan of Merger and Reorganization (the “Merger Agreement”), dated as of June 9, 2020, by and among Adgero Acquisition Corp., our wholly-owned subsidiary incorporated in the State of Delaware (“Merger Sub”), and Adgero. On August 19, 2020, upon the terms and subject to the conditions set forth in the Merger Agreement, Merger Sub merged with and into Adgero (the “Merger”), the separate corporate existence of Merger Sub ceased and Adgero continued its existence under Delaware law as the surviving corporation in the Merger and became our direct, wholly-owned subsidiary. As a result of the Merger, each issued and outstanding share of Adgero common stock, par value $0.0001 per share (the “Adgero Common Stock”) (other than treasury shares held by Adgero), was converted automatically into the right to receive 1.5740 shares (the “Exchange Ratio”) of our common stock, and cash in lieu of any fractional shares. Also, each outstanding warrant to purchase Adgero Common Stock was converted into a warrant exercisable for that number of shares of our common stock equal to the product of (x) the aggregate number of shares of Adgero Common Stock for which such warrant was exercisable and (y) the Exchange Ratio.
Following the completion of the Merger, we changed our name from DelMar Pharmaceuticals, Inc. to Kintara Therapeutics, Inc. In conjunction with the closing of the Merger, and through a series of three private placement closings, we issued a total of 25,028 shares of Series C Convertible Preferred Stock (the “Series C Stock”) at a purchase price of $1,000 per share for total aggregate gross proceeds of $25 million, or net proceeds of approximately $21.7 million.
The Series C Stock was issued in three series at conversion prices equal to $1.16, $1.214 and $1.15, respectively. As a result, we issued a total of 25,028 shares of Series C Stock, which are convertible into an aggregate 21,516,484 shares of common stock. As part of the private placement, we issued warrants to purchase 2,504 shares of Series C Stock to the placement agent (the “Placement Agent Warrants”). The Placement Agent Warrants have an exercise price of $1,000 per share, provide for a cashless exercise feature and are exercisable for a period of four years from the date of the initial closing of the private placement. The Series C Stock and the shares
62
of Series C Stock issuable upon exercise of the Placement Agent Warrants will be entitled to receive dividends, payable in shares of our common stock, at a rate of 10%, 15%, 20%, and 25%, of the number of shares of common stock issuable upon conversion of the Series C Stock, on the 12th, 24th, 36th and 48th month anniversary of the initial closing of the private placement, which occurred on August 19, 2020, provided that the holder of such shares has not converted the shares of Series C Stock prior to the applicable dividend rate.
Outstanding Securities
As of September 15, 2020, we had 23,543,892 shares of common stock issued and outstanding, outstanding, warrants to purchase 12,446,779 shares of common stock, warrants to purchase 2,504 Series C Preferred Stock that upon conversion are convertible into 2,152,667 shares of common stock, outstanding stock options to purchase 6,243,872 shares of common stock, 648,613 outstanding shares of Series B Preferred Stock that are convertible into 162,177 shares of common stock, 25,028 outstanding shares of Series C Preferred Stock that are convertible into 21,516,484 shares of common stock. All warrants and stock options are convertible, or exercisable into, one share of common stock. Each Series B convertible preferred share is convertible into 0.25 shares of common stock and the Series C convertible Preferred Stock (issued in three series) are convertible into a total of 21,516,484 shares of common stock
On May 8, 2019, we effected a one-for-ten reverse stock split (the “Reverse Stock Split”) of our issued and outstanding and authorized common stock. All per share amounts and number of shares of common stock in the MD&A and the consolidated financial statements reflect the Reverse Stock Split. The Reverse Stock Split does not affect the our authorized preferred stock of 5,000,000 shares; except that, pursuant to the terms of the Certificate of Designations of Series B Convertible Preferred Stock for the issued and outstanding shares of our Series B Convertible Preferred Stock, par value $0.001 per share (the “Series B Preferred Stock”), the conversion price at which shares of Series B Preferred Stock may be converted into shares of common stock will be proportionately adjusted to reflect the Reverse Stock Split.
On June 26, 2019, we amended our articles of incorporation, as amended, to increase the number of authorized shares of common stock from 7,000,000 to 95,000,000 shares.
Related Parties
We acquired our initial patents and technology rights from Valent, an entity owned by Dr. Dennis Brown, our Chief Scientific Officer. As a result, Valent is a related party to us.
Selected Annual Information
The financial information reported herein has been prepared in accordance with accounting principles generally accepted in the United States. Our functional currency at June 30, 2020 and June 30, 2019 is the US$. The following tables represent selected financial information for us for the periods presented.
Selected Balance Sheet data
|
|
|
June 30, 2020 |
|
|
June 30, 2019 |
|
||
|
|
|
$ |
|
|
$ |
|
||
|
Cash and cash equivalents |
|
|
2,392,402 |
|
|
|
3,718,758 |
|
|
Working capital |
|
|
176,161 |
|
|
|
1,955,468 |
|
|
Total assets |
|
|
2,938,137 |
|
|
|
4,037,255 |
|
|
Total stockholders’ equity |
|
|
263,214 |
|
|
|
1,967,530 |
|
63
Selected Statement of Operations data
For the years ended
|
|
|
June 30, 2020 |
|
|
June 30, 2019 |
|
||
|
|
|
$ |
|
|
$ |
|
||
|
Expenses |
|
|
|
|
|
|
|
|
|
Research and development |
|
|
3,630,024 |
|
|
|
3,662,056 |
|
|
General and administrative |
|
|
4,514,520 |
|
|
|
4,736,440 |
|
|
Merger costs |
|
|
1,053,697 |
|
|
|
— |
|
|
|
|
|
9,198,241 |
|
|
|
8,398,496 |
|
|
Other (income) loss |
|
|
|
|
|
|
|
|
|
Change in fair value of derivative liabilities |
|
|
— |
|
|
|
(433,503 |
) |
|
Derivative liability issue costs |
|
|
— |
|
|
|
126,186 |
|
|
Foreign exchange loss |
|
|
2,923 |
|
|
|
17,746 |
|
|
Interest income |
|
|
(75,248 |
) |
|
|
(60,704 |
) |
|
|
|
|
(72,325 |
) |
|
|
(350,275 |
) |
|
Net loss for the year |
|
|
9,125,916 |
|
|
|
8,048,221 |
|
|
Series B Preferred stock dividend |
|
|
8,616 |
|
|
|
80,431 |
|
|
Net loss for the year attributable to common stockholders |
|
|
9,134,532 |
|
|
|
8,128,652 |
|
|
Basic and fully diluted number of shares |
|
|
10,444,045 |
|
|
|
2,574,692 |
|
|
Basic and fully diluted loss per share |
|
|
0.87 |
|
|
|
3.16 |
|
Expenses net of non-cash, share-based compensation expense - non-GAAP
The following table discloses research and development, and general and administrative expenses net of non-cash, share-based compensation payment expense. The disclosure has been provided to reconcile the total operational expenses on a GAAP basis and the non-GAAP operational expenses net of non-cash stock-based compensation in order to provide an estimate of cash used in research and development, and general and administrative expense. Management uses the cash basis of expenses for forecasting and budget purposes to determine the allocation of resources and to plan for future financing opportunities.
For the years ended
|
|
|
June 30, 2020 $ |
|
|
June 30, 2019 $ |
|
||
|
Research and development – GAAP |
|
|
3,630,024 |
|
|
|
3,662,056 |
|
|
Less: non-cash share-based compensation expense |
|
|
(100,231 |
) |
|
|
(88,445 |
) |
|
Research and development net of non-cash share-based, compensation expense- Non-GAAP |
|
|
3,529,793 |
|
|
|
3,573,611 |
|
|
General and administrative – GAAP |
|
|
4,514,520 |
|
|
|
4,736,440 |
|
|
Less: non-cash share-based compensation expense |
|
|
(601,508 |
) |
|
|
(901,218 |
) |
|
General and administrative net of non-cash share-based, compensation expense – Non-GAAP |
|
|
3,913,012 |
|
|
|
3,835,222 |
|
64
Comparison of the years ended June 30, 2020 and June 30, 2019
|
|
|
Years ended |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
June 30, 2020 $ |
|
|
June 30, 2019 $ |
|
|
Change $ |
|
|
Change % |
|
||||
|
Expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
3,630,024 |
|
|
|
3,662,056 |
|
|
|
(32,032 |
) |
|
|
(1 |
) |
|
General and administrative |
|
|
4,514,520 |
|
|
|
4,736,440 |
|
|
|
(221,920 |
) |
|
|
(5 |
) |
|
Merger costs |
|
|
1,053,697 |
|
|
|
— |
|
|
|
1,053,697 |
|
|
|
100 |
|
|
|
|
|
9,198,241 |
|
|
|
8,398,496 |
|
|
|
799,745 |
|
|
|
|
|
|
Other (income) loss |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Change in fair value of derivative liabilities |
|
|
— |
|
|
|
(433,503 |
) |
|
|
433,503 |
|
|
|
100 |
|
|
Derivative liability issue costs |
|
|
— |
|
|
|
126,186 |
|
|
|
(126,186 |
) |
|
|
(100 |
) |
|
Foreign exchange loss |
|
|
2,923 |
|
|
|
17,746 |
|
|
|
(14,823 |
) |
|
|
(84 |
) |
|
Interest income |
|
|
(75,248 |
) |
|
|
(60,704 |
) |
|
|
(14,544 |
) |
|
|
24 |
|
|
|
|
|
(72,325 |
) |
|
|
(350,275 |
) |
|
|
277,950 |
|
|
|
|
|
|
Net loss |
|
|
9,125,916 |
|
|
|
8,048,221 |
|
|
|
1,077,695 |
|
|
|
|
|
Research and Development
Research and development expenses decreased slightly to $3,630,024 for the year ended June 30, 2020 from $3,662,056 for the year ended June 30, 2019. The decrease was largely attributable to lower preclinical research, personnel, and intellectual property expenses partially offset by higher clinical development costs in the current year compared to the prior year.
Preclinical research costs decreased during the year ended June 30, 2020 compared to the year ended June 30, 2019 due to the completion, or deferral, of studies that were ongoing in the prior year as well as us focusing our resources on our clinical studies in the current year. Personnel costs have decreased in the year ended June 30, 2020 compared to the year ended June 30, 2019 due a reduction in full-time employee head count in the current year compared to the prior year. Intellectual property costs decreased in the year ended June 30, 2020 compared to the year ended June 30, 2019 as we have refined our patent portfolio by focusing on our most important patent claims in the most strategic jurisdictions. Patent costs can vary considerably depending on the filing of new patents, conversion of the provisional applications to PCT applications, foreign office actions, and actual filing costs.
Clinical development costs increased in the year ended June 30, 2020 largely due to the initial costs we have incurred related to the GCAR GBM AGILE study. In June 2020 we announced our acceptance of an invitation from GCAR to include VAL-083 in GCAR's GBM AGILE study, an adaptive clinical study platform in GBM. Upon acceptance, we incurred certain costs to initiate the preliminary agreement. We expect our research and development costs to increase in fiscal 2021 as our GCAR GBM AGILE study commences. In addition, our planned clinical study for REM-001 is expected to commence in the coming year.
General and Administrative
General and administrative expenses were $4,514,520 for the year ended June 30, 2020 compared to $4,736,440 for the year ended June 30, 2019. A significant portion of the decrease was due to lower professional fees and non-cash, share-based compensation expense partially offset by higher office and sundry expenses in the current year compared to the prior year.
Professional fees decreased during the year ended June 30, 2020 compared to the year ended June 30, 2019 primarily due to our proposed rights offering in the prior year which was terminated in June 2019. As a result, the professional fees related to the Rights Offering of $555,664 were expensed in the quarter ended June 30, 2019. Office and sundry has increased in the year ended June 30, 2020 compared to the year ended June 30, 2019 due primarily to costs of higher directors’ and officers’ liability insurance.
In relation to general and administrative expenses during the year ended June 30, 2020, we incurred non-cash, share-based compensation expense relating to warrants issued for services and stock option expense while during the year ended June 30, 2019, we incurred non-cash, share-based compensation expense relating to performance share units, warrants issued for services, and stock option expense. All performance share units were canceled on April 30, 2019 so there was no related expense incurred during the year ended June 30, 2020.
65
Merger costs
Merger costs of $1,053,697 (2019 - $Nil) relate to expenditures incurred prior to June 30, 2020 with respect to the Adgero Merger and have been expensed.
Preferred Share Dividends
For each of the years ended June 30, 2020 and 2019 we recorded $8,356 related to the dividend payable to Valent on the Series A preferred stock. The dividend has been recorded as a direct increase in accumulated deficit for both years.
During the year ended June 30, 2020, we issued 14,800 (2019 – 18,271) shares of common stock as a dividend on the Series B Preferred stock and recognized $8,616 (2019 - $80,431) as a direct increase in accumulated deficit.
Liquidity and Capital Resources
Comparison of the years ended June 30, 2020 and June 30, 2019
|
|
|
June 30, 2020 $ |
|
|
June 30, 2019 $ |
|
|
Change $ |
|
|
Change % |
|
||||
|
Cash flows from operating activities |
|
|
(7,927,516 |
) |
|
|
(6,327,425 |
) |
|
|
(1,600,091 |
) |
|
|
25 |
|
|
Cash flows from financing activities |
|
|
6,601,160 |
|
|
|
4,074,188 |
|
|
|
2,526,972 |
|
|
|
62 |
|
Operating Activities
Net cash used in operating activities increased to $7,927,516 for the year ended June 30, 2020 from $6,327,425 for the year ended June 30, 2019. During the year ended June 30, 2020 and 2019 we reported net losses of $9,125,916 and $8,048,221, respectively. Changes in adjustments to reconcile net loss to net cash used in operating activities for the year ended June 30, 2020 compared to June 30, 2019 included higher warrants issued for services in the current year due to more warrants being issued in the current year compared to the prior year. Items incurred during the year ended June 30, 2019 but not in the year ended June 30, 2020 include a change in the fair value of derivative liabilities of $433,503 and performance stock unit expense of $526,141. The most significant changes in working capital for the year ended June 30, 2020 were from uses of cash due to an increase in non-financing related accounts payable and accrued liabilities of $206,597, an increase in related party payables of $338,657, and an increase in prepaid expenses of $75,332. The most significant change in working capital for the year ended June 30, 2019 was cash from a reduction in prepaid expenses and deposits of $754,682 largely due to a partial refund of a clinical study deposit, and cash from an increase in accounts payable and accrued liabilities of $202,000.
Financing Activities
During the year ended June 30, 2020, we received $6,582,966 in net proceeds from the completion of an underwritten public offering by us of common stock, pre-funded warrants, and common stock purchase warrants. Additionally, we received $51,550 pursuant to the exercise of warrants in the current year. At June 30, 2020, we have incurred $25,000 in deferred financing costs, net of deferred financing costs included in accounts payable, related to the private placement completed in August 2020.
During the year ended June 30, 2019, we received $3,362,379 in net proceeds from the completion of a registered direct offering by us of common stock and common stock purchase warrants. We also received $720,165 in net proceeds from the exercise and exchange of warrants.
Liquidity Risk and Capital Expenditure Requirements
Liquidity Risk
(See note 1 to the consolidated financial statements)
The consolidated financial statements have been prepared on a going concern basis which assumes that we will continue our operations for the foreseeable future and contemplates the realization of assets and the settlement of liabilities in the normal course of business.
66
For the year ended June 30, 2020, we reported a loss of $9,125,916, and a negative cash flow from operations of $7,927,516. We had an accumulated deficit of $69,721,233 as of June 30, 2020. As of June 30, 2020, we had cash and cash equivalents on hand of $2,392,402. We are in the clinical stage and have not generated any revenues to-date. We do not have the prospect of achieving revenues until such time that our product candidates are commercialized, or partnered, which may not ever occur. In the future, we will require additional funding to maintain our clinical studies, research and development projects, and for general operations. We may tailor the development programs of our drug candidates based on the amount of funding we are able to raise in the future.
These circumstances had indicated substantial doubt existed about our ability to continue as a going concern. Subsequent to June 30, 2020, we completed a private placement in three closings for gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million. We believe that based on our current estimates, cash on hand at June 30, 2020 and the proceeds from the private placement, will be sufficient to fund our planned operations beyond the next year from the date the consolidated financial statements are issued. As a result, substantial doubt about our ability to continue as a going concern has been alleviated. However, the COVID-19 pandemic has created significant economic uncertainty and volatility in the credit and capital markets. The ultimate impact of the COVID-19 pandemic on our ability to raise additional capital in the future is unknown and will depend on future developments, which are highly uncertain and cannot be predicted with confidence, including the duration of the COVID-19 outbreak and any new information which may emerge concerning the severity of the COVID-19 pandemic.
The financial statements do not give effect to any adjustments to the amounts and classification of assets and liabilities that may be necessary should we be unable to continue as a going concern. Such adjustments could be material.
Our future funding requirements will depend on many factors, including but not limited to:
|
|
• |
the rate of progress and cost of our clinical studies, preclinical studies and other discovery and research and development activities; |
|
|
• |
the costs associated with establishing manufacturing and commercialization capabilities; |
|
|
• |
the costs of acquiring or investing in businesses, product candidates and technologies; |
|
|
• |
the costs of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights; |
|
|
• |
the costs and timing of seeking and obtaining FDA and other regulatory approvals; |
|
|
• |
the effect of competing technological and market developments; |
|
|
• |
the economic and other terms and timing of any collaboration, licensing or other arrangements into which we may enter; and |
|
|
• |
the impact of us being a public entity. |
Until we can generate a sufficient amount of product revenue to finance our cash requirements, which we may never do, we expect to finance future cash needs primarily through public or private equity offerings, or strategic collaborations. The sale of equity and convertible debt securities may result in dilution to our stockholders and certain of those securities may have rights senior to those of our shares of capital stock. If we raise additional funds through the issuance of preferred stock, convertible debt securities or other debt financing, these securities or other debt could contain covenants that would restrict our operations. Any other third-party funding arrangement could require us to relinquish valuable rights. Economic conditions may affect the availability of funds and activity in equity markets. We do not know whether additional funding will be available on acceptable terms, or at all. If we are not able to secure additional funding when needed, we may have to delay, reduce the scope of or eliminate one or more of our clinical trials or research and development programs or make changes to our operating plan. In addition, we may have to seek a partner for one or more of our product candidates at an earlier stage of development, which would lower the economic value of those programs to us.
Critical Accounting Policies
The preparation of financial statements, in conformity with generally accepted accounting principles in the United States, requires companies to establish accounting policies and to make estimates that affect both the amount and timing of the recording of assets, liabilities, revenues and expenses. Some of these estimates require judgments about matters that are inherently uncertain and therefore actual results may differ from those estimates.
67
A detailed presentation of all of our significant accounting policies and the estimates derived therefrom is included in Note 2 to our consolidated financial statements for the year ended June 30, 2020 contained elsewhere in this report on Form 10-K. While all of the significant accounting policies are important to our consolidated financial statements, the following accounting policies and the estimates derived therefrom are critical:
|
|
• |
Warrants and shares issued for services |
|
|
• |
Stock options |
|
|
• |
Accruals for research and development expenses and clinical trials |
Warrants and shares issued for services
We have issued equity instruments for services provided by employees and nonemployees. The equity instruments are valued at the fair value of the instrument granted.
Stock options
We recognize compensation costs resulting from the issuance of stock-based awards to employees, non-employees and directors as an expense in the statement of operations over the service period based on a measurement of fair value for each stock-based award. Prior to our adoption of ASU 2018-07, Compensation-Stock Compensation (Topic 718), Improvements to Nonemployee Share-Based Payment Accounting (“ASU 2018-07”), stock options granted to non-employee consultants were revalued at the end of each reporting period until vested using the Black-Scholes option-pricing model and the changes in their fair value were recorded as adjustments to expense over the related vesting period. For the year ended June 30, 2019, the determination of grant-date fair value for stock option awards was estimated using the Black-Scholes model, which includes variables such as the expected volatility of our share price, the anticipated exercise behavior of its grantee, interest rates, and dividend yields. For the year ended June 30, 2020, we utilized the plain vanilla method to determine the expected life of stock options. These variables are projected based on our historical data, experience, and other factors. Changes in any of these variables could result in material adjustments to the expense recognized for share-based payments. Such value is recognized as expense over the requisite service period, net of actual forfeitures, using the accelerated attribution method. We recognize forfeitures as they occur. The estimation of stock awards that will ultimately vest requires judgment, and to the extent actual results, or updated estimates, differ from current estimates, such amounts are recorded as a cumulative adjustment in the period estimates are revised.
Accruals for research and development expenses and clinical trials
As part of the process of preparing our financial statements, we are required to estimate our expenses resulting from our obligations under contracts with vendors, clinical research organizations and consultants, and under clinical site agreements in connection with conducting clinical trials. The financial terms of these contracts are subject to negotiations, which vary from contract to contract and may result in payment terms that do not match the periods over which materials or services are provided under such contracts. Our objective is to reflect the appropriate expenses in our financial statements by matching those expenses with the period in which services are performed and efforts are expended. We account for these expenses according to the timing of various aspects of the expenses. We determine accrual estimates by taking into account discussion with applicable personnel and outside service providers as to the progress of clinical trials, or the services completed. During the course of a clinical trial, we adjust our clinical expense recognition if actual results differ from our estimates. We make estimates of our accrued expenses as of each balance sheet date based on the facts and circumstances known to us at that time. Our clinical trial accruals are dependent upon the timely and accurate reporting of contract research organizations and other third-party vendors. Although we do not expect our estimates to be materially different from amounts actually incurred, our understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in us reporting amounts that are too high or too low for any particular period. For years ended June 30, 2020 and 2019, there were no material adjustments to our prior period estimates of accrued expenses for clinical trials.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
Not required for a smaller reporting company.
68
Item 8. Financial Statements and Supplementary Data
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Consolidated Financial Statements
For the year ended June 30, 2020
(expressed in US dollars unless otherwise noted)
69
Report of Independent Registered Public Accounting Firm
To the Shareholders and Board of Directors of
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.) (the “Company”) as of June 30, 2020, the related consolidated statements of operations, stockholders’ equity and cash flows for the year then ended, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of June 30, 2020, and the results of its operations and its cash flows for the year then ended, in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's financial statements based on our audit. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) ("PCAOB") and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audit, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audit included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audit also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audit provides a reasonable basis for our opinion.
/s/ Marcum llp
Marcum llp
We have served as the Company’s auditor since 2019.
San Francisco, CA
September 18, 2020
70
Report of Independent Registered Public Accounting Firm
To the Shareholders and the Board of Directors of Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheet of Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.) (the “Company”) as of June 30, 2019, the related consolidated statements of operations, changes in stockholders’ equity and cash flows for the year then ended, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of June 30, 2019, and the results of its operations and its cash flows for the year then ended in conformity with U.S. generally accepted accounting principles.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audit. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the US federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audit, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audit included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures include examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audit also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audit provides a reasonable basis for our opinion.
/s/ Ernst & Young LLP
We served as the Company’s auditor from 2016 to 2019.
Vancouver, Canada
September 9, 2019
71
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
(expressed in US dollars unless otherwise noted)
|
|
|
|
|
|
|
As of June 30, |
|
|||||
|
|
|
|
|
|
|
2020 |
|
|
2019 |
|
||
|
|
|
Note |
|
|
$ |
|
|
$ |
|
|||
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Current assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
|
|
|
|
|
2,392,402 |
|
|
|
3,718,758 |
|
|
Prepaid expenses and deposits |
|
|
8 |
|
|
|
355,580 |
|
|
|
280,248 |
|
|
Interest, taxes and other receivables |
|
|
|
|
|
|
9,401 |
|
|
|
26,187 |
|
|
Deferred loan costs |
|
|
3 |
|
|
|
93,701 |
|
|
|
— |
|
|
|
|
|
|
|
|
|
2,851,084 |
|
|
|
4,025,193 |
|
|
Intangible assets - net |
|
|
|
|
|
|
2,109 |
|
|
|
12,062 |
|
|
Deferred financing costs |
|
|
3 |
|
|
|
84,944 |
|
|
|
— |
|
|
Total assets |
|
|
|
|
|
|
2,938,137 |
|
|
|
4,037,255 |
|
|
Liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Current liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Accounts payable and accrued liabilities |
|
|
|
|
|
|
2,011,058 |
|
|
|
1,744,517 |
|
|
Related party payables |
|
|
4 |
|
|
|
663,865 |
|
|
|
325,208 |
|
|
Total liabilities |
|
|
|
|
|
|
2,674,923 |
|
|
|
2,069,725 |
|
|
Stockholders’ equity |
|
|
|
|
|
|
|
|
|
|
|
|
|
Preferred stock |
|
|
|
|
|
|
|
|
|
|
|
|
|
Authorized |
|
|
|
|
|
|
|
|
|
|
|
|
|
5,000,000 shares, $0.001 par value |
|
|
|
|
|
|
|
|
|
|
|
|
|
Issued and outstanding |
|
|
|
|
|
|
|
|
|
|
|
|
|
278,530 Series A shares at June 30, 2020 (June 30, 2019 – 278,530) |
|
4,6 |
|
|
|
278,530 |
|
|
|
278,530 |
|
|
|
648,613 Series B shares at June 30, 2020 (June 30, 2019 – 673,613) |
|
|
6 |
|
|
|
4,524,897 |
|
|
|
4,699,304 |
|
|
Zero special voting shares at June 30, 2020 (June 30, 2019 – 1) |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
Common stock |
|
|
|
|
|
|
|
|
|
|
|
|
|
Authorized |
|
|
|
|
|
|
|
|
|
|
|
|
|
95,000,000 shares at June 30, 2020 and June 30, 2019, $0.001 par value |
|
|
|
|
|
|
|
|
|
|
|
|
|
11,457,928 issued at June 30, 2020 (June 30, 2019 – 3,839,358) |
|
|
6 |
|
|
|
11,458 |
|
|
|
3,839 |
|
|
Additional paid-in capital |
|
|
6 |
|
|
|
56,624,048 |
|
|
|
50,954,741 |
|
|
Warrants |
|
|
6 |
|
|
|
8,524,336 |
|
|
|
6,588,283 |
|
|
Accumulated deficit |
|
|
|
|
|
|
(69,721,233 |
) |
|
|
(60,578,345 |
) |
|
Accumulated other comprehensive income |
|
|
|
|
|
|
21,178 |
|
|
|
21,178 |
|
|
Total stockholders’ equity |
|
|
|
|
|
|
263,214 |
|
|
|
1,967,530 |
|
|
Total liabilities and stockholders’ equity |
|
|
|
|
|
|
2,938,137 |
|
|
|
4,037,255 |
|
|
Nature of operations, corporate history, and liquidity risk (note 1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Commitments and contingencies (note 8) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subsequent events (note 11) |
|
|
|
|
|
|
|
|
|
|
|
|
The accompanying notes are an integral part of these consolidated financial statements.
72
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Consolidated Statements of Operations
(expressed in US dollars unless otherwise noted)
|
|
|
|
|
|
|
For the years ended June 30, |
|
|||||
|
|
|
Note |
|
|
2020 |
|
|
2019 |
|
|||
|
|
|
|
|
|
|
$ |
|
|
$ |
|
||
|
Expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
|
|
|
|
3,630,024 |
|
|
|
3,662,056 |
|
|
General and administrative |
|
|
|
|
|
|
4,514,520 |
|
|
|
4,736,440 |
|
|
Merger costs |
|
11 |
|
|
|
1,053,697 |
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
9,198,241 |
|
|
|
8,398,496 |
|
|
Other (income) loss |
|
|
|
|
|
|
|
|
|
|
|
|
|
Change in fair value of derivative liabilities |
|
5,6 |
|
|
|
— |
|
|
|
(433,503 |
) |
|
|
Derivative liability issue costs |
|
|
5 |
|
|
|
— |
|
|
|
126,186 |
|
|
Foreign exchange loss |
|
|
|
|
|
|
2,923 |
|
|
|
17,746 |
|
|
Interest income |
|
|
|
|
|
|
(75,248 |
) |
|
|
(60,704 |
) |
|
|
|
|
|
|
|
|
(72,325 |
) |
|
|
(350,275 |
) |
|
Net loss for the year |
|
|
|
|
|
|
9,125,916 |
|
|
|
8,048,221 |
|
|
Computation of basic loss per share |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss for the year |
|
|
|
|
|
|
9,125,916 |
|
|
|
8,048,221 |
|
|
Series B Preferred stock dividend |
|
|
6 |
|
|
|
8,616 |
|
|
|
80,431 |
|
|
Net loss for the year attributable to common stockholders |
|
|
|
|
|
|
9,134,532 |
|
|
|
8,128,652 |
|
|
Basic and fully diluted loss per share |
|
|
|
|
|
|
0.87 |
|
|
|
3.16 |
|
|
Basic and fully diluted weighted average number of shares |
|
|
|
|
|
|
10,444,045 |
|
|
|
2,574,692 |
|
The accompanying notes are an integral part of these consolidated financial statements.
73
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Consolidated Statements of Stockholders’ Equity
(expressed in US dollars unless otherwise noted)
For the years ended June 30, 2020 and 2019
|
|
|
Number of shares |
|
|
Common stock $ |
|
|
Additional paid-in capital $ |
|
|
Accumulated other comprehensive income $ |
|
|
Preferred stock $ |
|
|
Warrants $ |
|
|
Accumulated deficit $ |
|
|
Stockholders' equity $ |
|
||||||||
|
Balance - June 30, 2018 |
|
|
2,296,667 |
|
|
|
2,297 |
|
|
|
43,198,193 |
|
|
|
21,178 |
|
|
|
6,425,410 |
|
|
|
8,229,482 |
|
|
|
(52,441,337 |
) |
|
|
5,435,223 |
|
|
Issuance of shares and warrants - net of issue costs |
|
|
1,170,000 |
|
|
|
1,170 |
|
|
|
2,332,102 |
|
|
|
— |
|
|
|
— |
|
|
|
52,899 |
|
|
|
— |
|
|
|
2,386,171 |
|
|
Exercise and exchange of warrants |
|
|
296,667 |
|
|
|
297 |
|
|
|
2,930,565 |
|
|
|
— |
|
|
|
— |
|
|
|
(2,210,697 |
) |
|
|
— |
|
|
|
720,165 |
|
|
Conversion of Series B preferred stock to common stock |
|
|
51,876 |
|
|
|
52 |
|
|
|
1,447,524 |
|
|
|
— |
|
|
|
(1,447,576 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Reclassification of derivative liability to equity |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
492,884 |
|
|
|
— |
|
|
|
492,884 |
|
|
Shares issued for services |
|
|
3,444 |
|
|
|
3 |
|
|
|
13,774 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
13,777 |
|
|
Warrants issued for services |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
23,715 |
|
|
|
— |
|
|
|
23,715 |
|
|
Shares issued on reverse stock split |
|
|
2,433 |
|
|
|
2 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
2 |
|
|
Stock option expense |
|
|
— |
|
|
|
— |
|
|
|
426,029 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
426,029 |
|
|
Performance stock unit expense |
|
|
— |
|
|
|
— |
|
|
|
526,141 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
526,141 |
|
|
Series A preferred cash dividend |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(8,356 |
) |
|
|
(8,356 |
) |
|
Series B preferred stock dividend |
|
|
18,271 |
|
|
|
18 |
|
|
|
80,413 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(80,431 |
) |
|
|
— |
|
|
Loss for the year |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(8,048,221 |
) |
|
|
(8,048,221 |
) |
|
Balance - June 30, 2019 |
|
|
3,839,358 |
|
|
|
3,839 |
|
|
|
50,954,741 |
|
|
|
21,178 |
|
|
|
4,977,834 |
|
|
|
6,588,283 |
|
|
|
(60,578,345 |
) |
|
|
1,967,530 |
|
|
Issuance of shares and warrants - net of issue costs |
|
|
4,895,000 |
|
|
|
4,895 |
|
|
|
2,489,251 |
|
|
|
— |
|
|
|
— |
|
|
|
4,088,820 |
|
|
|
— |
|
|
|
6,582,966 |
|
|
Exercise of pre-funded warrants for cash |
|
|
2,655,000 |
|
|
|
2,655 |
|
|
|
2,421,830 |
|
|
|
— |
|
|
|
— |
|
|
|
(2,397,935 |
) |
|
|
— |
|
|
|
26,550 |
|
|
Exercise of warrants for cash |
|
|
25,000 |
|
|
|
25 |
|
|
|
37,113 |
|
|
|
— |
|
|
|
— |
|
|
|
(12,138 |
) |
|
|
— |
|
|
|
25,000 |
|
|
Conversion of Series B preferred stock to common stock |
|
|
6,250 |
|
|
|
6 |
|
|
|
174,401 |
|
|
|
— |
|
|
|
(174,407 |
) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
Shares issued for services |
|
|
22,520 |
|
|
|
23 |
|
|
|
13,373 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
13,396 |
|
|
Warrants issued for services |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
287,183 |
|
|
|
— |
|
|
|
287,183 |
|
|
Warrants expired |
|
|
— |
|
|
|
— |
|
|
|
29,877 |
|
|
|
— |
|
|
|
— |
|
|
|
(29,877 |
) |
|
|
— |
|
|
|
— |
|
|
Stock option expense |
|
|
— |
|
|
|
— |
|
|
|
494,861 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
494,861 |
|
|
Series A preferred cash dividend |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(8,356 |
) |
|
|
(8,356 |
) |
|
Series B preferred stock dividend |
|
|
14,800 |
|
|
|
15 |
|
|
|
8,601 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(8,616 |
) |
|
|
— |
|
|
Loss for the year |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
(9,125,916 |
) |
|
|
(9,125,916 |
) |
|
Balance - June 30, 2020 |
|
|
11,457,928 |
|
|
|
11,458 |
|
|
|
56,624,048 |
|
|
|
21,178 |
|
|
|
4,803,427 |
|
|
|
8,524,336 |
|
|
|
(69,721,233 |
) |
|
|
263,214 |
|
The accompanying notes are an integral part of these consolidated financial statements.
74
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Consolidated Statements of Cash Flows
June 30, 2020
(expressed in US dollars unless otherwise noted)
|
|
|
|
|
|
|
For the years ended June 30, |
|
|||||
|
|
|
|
|
|
|
2020 |
|
|
2019 |
|
||
|
|
|
Note |
|
|
$ |
|
|
$ |
|
|||
|
Cash flows from operating activities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Loss for the year |
|
|
|
|
|
|
(9,125,916 |
) |
|
|
(8,048,221 |
) |
|
Adjustments to reconcile net loss to net cash used in operating activities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Non-cash derivative issue costs |
|
|
|
|
|
|
— |
|
|
|
13,495 |
|
|
Amortization of intangible assets |
|
|
|
|
|
|
9,953 |
|
|
|
16,349 |
|
|
Change in fair value of derivative liabilities |
|
5,6 |
|
|
|
— |
|
|
|
(433,503 |
) |
|
|
Shares issued for services |
|
|
6 |
|
|
|
13,396 |
|
|
|
13,777 |
|
|
Warrants issued for services |
|
|
6 |
|
|
|
193,482 |
|
|
|
23,715 |
|
|
Stock option expense |
|
|
6 |
|
|
|
494,861 |
|
|
|
426,029 |
|
|
Performance stock unit expense |
|
|
6 |
|
|
|
— |
|
|
|
526,141 |
|
|
Changes in operating assets and liabilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Prepaid expenses and deposits |
|
|
8 |
|
|
|
(75,332 |
) |
|
|
754,682 |
|
|
Interest, taxes and other receivables |
|
|
|
|
|
|
16,786 |
|
|
|
13,332 |
|
|
Accounts payable and accrued liabilities |
|
|
|
|
|
|
206,597 |
|
|
|
202,000 |
|
|
Related party payables |
|
|
|
|
|
|
338,657 |
|
|
|
164,779 |
|
|
Net cash used in operating activities |
|
|
|
|
|
|
(7,927,516 |
) |
|
|
(6,327,425 |
) |
|
Cash flows from financing activities |
|
|
|
|
|
|
|
|
|
|
|
|
|
Net proceeds from the issuance of shares and warrants |
|
|
6 |
|
|
|
6,582,966 |
|
|
|
3,362,379 |
|
|
Net proceeds from the exercise and exchange of warrants |
|
|
6 |
|
|
|
51,550 |
|
|
|
720,165 |
|
|
Series A preferred stock dividend |
|
|
4 |
|
|
|
(8,356 |
) |
|
|
(8,356 |
) |
|
Deferred financing costs |
|
3,9 |
|
|
|
(25,000 |
) |
|
|
— |
|
|
|
Net cash provided by financing activities |
|
|
|
|
|
|
6,601,160 |
|
|
|
4,074,188 |
|
|
Decrease in cash and cash equivalents |
|
|
|
|
|
|
(1,326,356 |
) |
|
|
(2,253,237 |
) |
|
Cash and cash equivalents – beginning of year |
|
|
|
|
|
|
3,718,758 |
|
|
|
5,971,995 |
|
|
Cash and cash equivalents – end of year |
|
|
|
|
|
|
2,392,402 |
|
|
|
3,718,758 |
|
|
Supplementary information (note 9) |
|
|
|
|
|
|
|
|
|
|
|
|
The accompanying notes are an integral part of these consolidated financial statements.
75
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.)
Notes to Consolidated Financial Statements
June 30, 2020
(expressed in US dollars unless otherwise noted)
|
1 |
Nature of operations, corporate history, and liquidity risk |
Nature of operations
Kintara Therapeutics, Inc. (formerly DelMar Pharmaceuticals, Inc.) (the “Company”) is a clinical stage drug development company with a focus on the development of novel cancer therapies for patients with unmet medical needs. The Company is developing two late-stage, Phase 3-ready therapeutics - VAL-083 for glioblastoma multiforme and REM-001 for cutaneous metastatic breast cancer. In order to accelerate the Company’s development timelines, it leverages existing preclinical and clinical data from a wide range of sources. The Company may seek marketing partnerships in order to potentially offset clinical costs and to generate future royalty revenue from approved indications of its product candidates.
Corporate history
The Company is a Nevada corporation formed on June 24, 2009 under the name Berry Only, Inc. On January 25, 2013, the Company entered into and closed an exchange agreement (the “Exchange Agreement”), with Del Mar Pharmaceuticals (BC) Ltd. (“Del Mar (BC)”), 0959454 B.C. Ltd. (“Callco”), and 0959456 B.C. Ltd. (“Exchangeco”) and the security holders of Del Mar (BC). Upon completion of the Exchange Agreement, Del Mar (BC) became a wholly-owned subsidiary of the Company (the “Reverse Acquisition”).
On August 19, 2020 the Company completed its merger with Adgero Biopharmaceuticals Holdings, Inc. (“Adgero”). In conjunction with the Adgero merger, the Company changed its name to Kintara Therapeutics, Inc.
Kintara Therapeutics, Inc. is the parent company of Del Mar (BC), a British Columbia, Canada corporation and Adgero, a Delaware corporation, which are clinical stage companies with a focus on the development of drugs for the treatment of cancer. The Company is also the parent company to Callco and Exchangeco which are British Columbia, Canada corporations. Callco and Exchangeco were formed to facilitate the Reverse Acquisition. In connection with the merger, the Company also became the parent company of Adgero Biopharmaceuticals, Inc., formerly a wholly-owned subsidiary of Adgero.
References to the Company refer to the Company and its wholly-owned subsidiaries.
Liquidity risk and management plans
These consolidated financial statements have been prepared on a going concern basis which assumes that the Company will continue its operations for the foreseeable future and contemplates the realization of assets and the settlement of liabilities in the normal course of business.
For the year ended June 30, 2020, the Company reported a loss of $9,125,916, and a negative cash flow from operations of $7,927,516. The Company had an accumulated deficit of $69,721,233 as of June 30, 2020. As of June 30, 2020, the Company has cash and cash equivalents on hand of $2,392,402. The Company is in the clinical stage and has not generated any revenues to-date. The Company does not have the prospect of achieving revenues until such time that its product candidates are commercialized, or partnered, which may not ever occur. In the future, the Company will require additional funding to maintain its clinical trials, research and development projects, and for general operations. The Company may tailor its drug development programs based on the amount of funding the Company is able to raise in the future.
These circumstances had indicated substantial doubt existed about the Company’s ability to continue as a going concern. Subsequent to June 30, 2020, the Company completed a private placement in three closings for gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million (note 11). The Company believes that based on its current estimates, the cash on hand at June 30, 2020 of $2,392,402 and the proceeds from the private placement, will be sufficient to fund its planned operations beyond the next year from the date these consolidated financial statements are issued. As a result, substantial doubt about the Company’s ability to continue as a going concern has been alleviated. However, the coronavirus (“COVID-19”) pandemic has created significant economic uncertainty and volatility in the credit and capital markets. The ultimate impact of the COVID-19 pandemic on the Company’s ability to raise additional capital in the future is unknown and will depend on future developments, which are highly uncertain and cannot be predicted with confidence, including the duration of the COVID-19 outbreak and any new information which may emerge concerning the severity of the COVID-19 pandemic.
76
These financial statements do not give effect to any adjustments to the amounts and classification of assets and liabilities that may be necessary should the Company be unable to continue as a going concern. Such adjustments could be material.
|
2 |
Significant accounting policies |
Reverse stock split
On May 7, 2019, the Company filed a Certificate of Change with the Secretary of State of Nevada that effected a 1-for-10 (1:10) reverse stock split of its common stock, par value $0.001 per share, which became effective on May 8, 2019. Pursuant to the Certificate of Change, the Company’s authorized common stock was decreased in the same proportion as the split resulting in a decrease from 70,000,000 authorized shares of common stock to 7,000,000 shares authorized. The par value of its common stock was unchanged at $0.001 per share, post-split. All common shares, warrants, stock options, conversion ratios, and per share information in these consolidated financial statements give retroactive effect to the 1-for-10 reverse stock split. The Company’s authorized and issued preferred stock was not affected by the split.
Amended articles of incorporation
On June 26, 2019, the Company amended its articles of incorporation to increase the number of authorized shares of common stock from 7,000,000 to 95,000,000 shares.
Basis of presentation
The consolidated financial statements of the Company have been prepared in accordance with United States Generally Accepted Accounting Principles (“U.S. GAAP”) and are presented in United States dollars. The functional currency of the Company and each of its subsidiaries is the United States dollar.
The principal accounting policies applied in the preparation of these consolidated financial statements are set out below and have been consistently applied to all years presented.
Consolidation
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiaries, Del Mar BC, Callco, and Exchangeco as of and for the years ended June 30, 2020 and 2019. Intercompany balances and transactions have been eliminated on consolidation.
Use of estimates
The preparation of financial statements in conformity with US GAAP requires management to make estimates and assumptions about future events that affect the reported amounts of assets, liabilities, expenses, contingent assets, and contingent liabilities as at the end of, or during, the reporting period. Actual results could significantly differ from those estimates. Significant areas requiring management to make estimates include the fair value of the derivative liabilities, the valuation of equity instruments issued for services, and clinical trial accruals. Further details of the nature of these assumptions and conditions may be found in the relevant notes to these consolidated financial statements.
Cash and cash equivalents
Cash and cash equivalents consist of cash and highly liquid investments with original maturities from the purchase date of three months or less that can be readily convertible into known amounts of cash. Cash and cash equivalents are held at recognized Canadian and United States financial institutions. Interest earned is recognized in the consolidated statement of operations.
Foreign currency translation
The functional currency of the Company at June 30, 2020 is the United States dollar. Transactions that are denominated in a foreign currency are remeasured into the functional currency at the current exchange rate on the date of the transaction. Any foreign-currency denominated monetary assets and liabilities are subsequently remeasured at current exchange rates, with gains or losses recognized as foreign exchange losses or gains in the consolidated statement of operations. Non-monetary assets and liabilities are translated at historical exchange rates. Expenses are translated at average exchange rates during the period. Exchange gains and losses are included in consolidated statement of operations for the period.
77
Income taxes
The Company uses the asset and liability method of accounting for income taxes. Deferred tax assets and liabilities are recognized for the estimated future tax consequences attributable to the differences between the consolidated financial statement carrying amounts of existing assets and liabilities and their respective tax bases. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. To the extent that deferred tax assets cannot be recognized under the preceding criteria, the Company establishes valuation allowances, as necessary, to reduce deferred tax assets to the amounts expected to be realized.
As of June 30, 2020, and 2019, all deferred tax assets were fully offset by a valuation allowance. The realization of deferred tax assets is dependent upon future federal, state and foreign taxable income. The Company’s judgments regarding deferred tax assets may change due to future market conditions, as the Company expands into international jurisdictions, due to changes in U.S. or international tax laws and other factors.
These changes, if any, may require material adjustments to the Company’s deferred tax assets, resulting in a reduction in net income or an increase in net loss in the period in which such determinations are made. The Company recognizes the impact of uncertain tax positions based upon a two-step process. To the extent that a tax position does not meet a more-likely-than-not level of certainty, no impact is recognized in the consolidated financial statements. If a tax position meets the more-likely-than-not level of certainty, it is recognized in the consolidated financial statements at the largest amount that has a greater than 50% likelihood of being realized upon ultimate settlement. The Company’s policy is to analyze the Company’s tax positions taken with respect to all applicable income tax issues for all open tax years in each respective jurisdiction. Interest and penalties with respect to uncertain tax positions would be included in income tax expense. As of June 30, 2020, the Company concluded that there were no uncertain tax provisions required to be recognized in its consolidated financial statements.
The Company does not record U.S. income taxes on the undistributed earnings of its foreign subsidiaries based upon the Company’s intention to permanently reinvest undistributed earnings to ensure sufficient working capital and further expansion of existing operations outside the United States. As June 30, 2020, the Company’s foreign subsidiaries operated at a cumulative deficit for U.S. earnings and profit purposes. In the event the Company is required to repatriate funds from outside of the United States, such repatriation would be subject to local laws, customs, and tax consequences. Determination of the amount of unrecognized deferred tax liability related to these earnings is not practicable.
Financial instruments
The Company has financial instruments that are measured at fair value. To determine the fair value, the Company uses the fair value hierarchy for inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the most observable inputs be used when available. Observable inputs are inputs market participants would use to value an asset or liability and are developed based on market data obtained from independent sources. Unobservable inputs are inputs based on assumptions about the factors market participants would use to value an asset or liability. The three levels of inputs that may be used to measure fair value are as follows:
|
|
• |
Level one - inputs utilize quoted prices (unadjusted) in active markets for identical assets or liabilities; |
|
|
• |
Level two - inputs are inputs other than quoted prices included in Level 1 that are observable for the asset or liability, either directly or indirectly such as interest rates, foreign exchange rates, and yield curves that are observable at commonly quoted intervals; and |
|
|
• |
Level three - unobservable inputs developed using estimates and assumptions, which are developed by the reporting entity and reflect those assumptions that a market participant would use. |
Assets and liabilities are classified based on the lowest level of input that is significant to the fair value measurements. Changes in the observability of valuation inputs may result in a reclassification of levels for certain securities within the fair value hierarchy. As of June 30, 2020, and 2019, the Company had certain derivative liabilities under the fair value hierarchy but their fair value was zero.
The Company’s financial instruments consist of cash and cash equivalents, prepaid expenses, taxes and other receivables, accounts payable and accrued liabilities, related party payables and derivative liabilities. The carrying values of cash and cash equivalents, taxes and other receivables, accounts payable and accrued liabilities, and related party payables approximate their fair values due to the immediate, or short-term, maturity of these financial instruments.
78
Derivative liabilities
The Company accounts for certain warrants under the authoritative guidance on accounting for derivative financial instruments indexed to, and potentially settled in, a company’s own stock, on the understanding that in compliance with applicable securities laws, the warrants require the issuance of securities upon exercise and do not sufficiently preclude an implied right to net cash settlement, or contain a repricing feature under certain conditions. The Company classifies these warrants on its balance sheet as a derivative liability which is fair valued at each reporting period subsequent to the initial issuance. The Company has used a Black-Scholes Option Pricing Model (based on a closed-form model that uses a fixed equation) to estimate the fair value of the share warrants. Determining the appropriate fair-value model and calculating the fair value of warrants requires considerable judgment. Any change in the estimates (specifically probabilities and volatility) used may cause the value to be higher or lower than that reported. The estimated volatility of the Company’s common stock at the date of issuance, and at each subsequent reporting period, is based on the historical volatility of the Company. The risk-free interest rate is based on rates published by the government for bonds with a maturity similar to the expected remaining life of the warrants at the valuation date. The expected life of the warrants is assumed to be equivalent to their remaining contractual term.
The derivative is not traded in an active market and the fair value is determined using valuation techniques. The Company uses judgment to select a variety of methods to make assumptions that are based on specific management plans and market conditions at the end of each reporting period. The Company uses a fair value estimate to determine the fair value of the derivative liabilities. The carrying value of the derivative liabilities would be higher, or lower, as management estimates around specific probabilities change. The estimates may be significantly different from those amounts ultimately recorded in the consolidated financial statements because of the use of judgment and the inherent uncertainty in estimating the fair value of these instruments that are not quoted in an active market. All changes in the fair value are recorded in the consolidated statement of operations each reporting period. This is considered to be a Level 3 financial instrument as volatility is considered a Level 3 input.
Intangible assets
Website development costs
Website development costs are stated at cost less accumulated amortization. The Company capitalizes website development costs associated with graphics design and development of the website application and infrastructure. Costs related to planning, content input, and website operations are expensed as incurred. The Company amortizes website development costs on a straight-line basis over three years. At June 30, 2020, the total capitalized cost was $79,910 (2019 - $79,910) and the Company has recognized $9,953 and $16,349, respectively, in amortization expense during the years ended June 30, 2020 and 2019.
Patents
Expenditures associated with the filing, or maintenance of patents, licensing or technology agreements are expensed as incurred. Costs previously recognized as an expense are not recognized as an asset in subsequent periods. Once the Company has achieved regulatory approval patent costs will be deferred and amortized over the remaining life of the related patent.
Accruals for research and development expenses and clinical trials
As part of the process of preparing its financial statements, the Company is required to estimate its expenses resulting from its obligations under contracts with vendors, clinical research organizations and consultants, and under clinical site agreements in connection with conducting clinical trials. The financial terms of these contracts are subject to negotiations, which vary from contract to contract and may result in payment terms that do not match the periods over which materials or services are provided under such contracts. The Company’s objective is to reflect the appropriate expenses in its financial statements by matching those expenses with the period in which services are performed and efforts are expended. The Company accounts for these expenses according to the timing of various aspects of the expenses. The Company determines accrual estimates by taking into account discussion with applicable personnel and outside service providers as to the progress of clinical trials, or the services completed. During the course of a clinical trial, the Company adjusts its clinical expense recognition if actual results differ from its estimates. The Company makes estimates of its accrued expenses as of each balance sheet date based on the facts and circumstances known to it at that time. The Company’s clinical trial accruals are dependent upon the timely and accurate reporting of contract research organizations and other third-party vendors. Although the Company does not expect its estimates to be materially different from amounts actually incurred, its understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in it reporting amounts that are too high or too low for any particular period. For the years ended June 30, 2020 and 2019, there were no material adjustments to the Company’s prior period estimates of accrued expenses for clinical trials.
79
Warrants and shares issued for services
The Company has issued equity instruments for services provided by employees and non-employees. The equity instruments are valued at the fair value of the instrument issued.
Stock options
The Company recognizes compensation costs resulting from the issuance of stock-based awards to employees, non-employees and directors as an expense in the statement of operations over the service period based on a measurement of fair value for each stock-based award. Prior to the Company’s adoption of ASU 2018-07, Compensation-Stock Compensation (Topic 718), Improvements to Nonemployee Share-Based Payment Accounting (“ASU 2018-07”), stock options granted to non-employee consultants were revalued at the end of each reporting period until vested using the Black-Scholes option-pricing model and the changes in their fair value were recorded as adjustments to expense over the related vesting period. For the year ended June 30, 2019, the determination of grant-date fair value for stock option awards was estimated using the Black-Scholes model, which includes variables such as the expected volatility of the Company’s share price, the anticipated exercise behavior of its grantee, interest rates, and dividend yields. For the year ended June 30, 2020, the Company utilized the plain vanilla method to determine the expected life of stock options. These variables are projected based on the Company’s historical data, experience, and other factors. Changes in any of these variables could result in material adjustments to the expense recognized for share-based payments. Such value is recognized as expense over the requisite service period, net of actual forfeitures, using the accelerated attribution method. The Company recognizes forfeitures as they occur. The estimation of stock awards that will ultimately vest requires judgment, and to the extent actual results, or updated estimates, differ from current estimates, such amounts are recorded as a cumulative adjustment in the period estimates are revised.
Performance stock units
The Company also accounts for performance stock units (PSUs) under ASC 718. ASC 718 requires measurement of compensation cost for all stock-based awards at fair value on the date of grant and recognition of compensation expense over the requisite service period for awards expected to vest. As vesting of the PSUs is based on a number of factors, the determination of the grant-date fair value for PSUs has been estimated using a Monte Carlo simulation approach which includes variables such as the expected volatility of the Company’s share price and interest rates to generate potential future outcomes. These variables are projected based on the Company’s historical data, experience, and other factors. Changes in any of these variables could result in material adjustments to the expense recognized for the PSUs. Such value is recognized as expense over the derived service period using the accelerated attribution method. The estimation of PSUs that will ultimately vest requires judgment, and to the extent actual results, or updated estimates, differ from current estimates, such amounts are recorded as a cumulative adjustment in the period estimates are revised.
Loss per share
Income or loss per share is calculated based on the weighted average number of common shares outstanding. For the years ended June 30, 2020 and 2019 diluted loss per share does not differ from basic loss per share since the effect of the Company’s warrants, stock options, performance stock units, and convertible preferred shares is anti-dilutive. As of June 30, 2020, potential common shares of 10,309,456 (2019 – 1,543,596) related to outstanding warrants, 1,559,199 (2019 – 288,183) related to stock options, and 162,177 (2019 – 168,427) relating to outstanding Series B convertible preferred shares were excluded from the calculation of net loss per common share.
Segment information
The Company identifies its operating segments based on business activities, management responsibility and geographical location. The Company operates within a single operating segment being the research and development of cancer indications, and operates primarily in one geographic area, being North America. The Company is conducting one clinical trial in China but the planned expenses to be incurred over the course of the study are not expected to be significant. All of the Company’s assets are located in either Canada or the United States.
80
Recent accounting pronouncements
From time to time, new accounting pronouncements are issued by the Financial Accounting Standards Board (“FASB”) or other standard setting bodies that are adopted by the Company as of the specified effective date.
Recently adopted
Accounting Standards Update (“ASU”) 2016-02 — Leases (Topic 842)
The new standard establishes a right-of-use (“ROU”) model that requires a lessee to record a ROU asset and a lease liability on the consolidated balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the consolidated income statement. ASU 2016-02 is effective for annual periods beginning after December 15, 2019, including interim periods within those annual periods, with early adoption permitted. A modified retrospective transition approach is required for lessees for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. The early adoption of ASU 2016-02 did not have a material impact on the Company’s consolidated financial statements.
ASU 2018-07 — Stock Compensation (Topic 718) Improvements to Nonemployee Shares-based Payment Accounting
The amendments in this update are intended to the reduce cost and complexity and to improve financial reporting for share-based payments issued to nonemployees. The ASU expands the scope of Topic 718, Compensation —Stock Compensation, which currently only includes share-based payments issued to employees, to also include share-based payments issued to nonemployees for goods and services. The existing guidance on nonemployee share-based payments is significantly different from current guidance for employee share-based payments. This ASU expands the scope of the employee share-based payments guidance to include share-based payments issued to nonemployees. By doing so, the FASB improves the accounting of nonemployee share-based payments issued to acquire goods and services used in its own operations. The amendments in this ASU are effective for public companies for fiscal years beginning after December 15, 2019, including interim periods within that fiscal year. The early adoption of ASU 2018-07 did not have a material impact on the Company’s consolidated financial statements.
ASU 2017-11 — I. Accounting for Certain Financial Instruments with Down Round Features, II. Replacement of the Indefinite Deferral for Mandatorily Redeemable Financial Instruments of Certain Non-public Entities and Certain Mandatorily Redeemable Noncontrolling Interests with a Scope Exception
The amendments in this update are intended to reduce the complexity associated with the accounting for certain financial instruments with characteristics of liabilities and equity. Specifically, a down round feature would no longer cause a freestanding equity-linked financial instrument (or an embedded conversion option) to be accounted for as a derivative liability at fair value with changes in fair value recognized in current earnings. In addition, the indefinite deferral of certain provisions of Topic 480 have been re-characterized to a scope exception. The re-characterization has no accounting effect. ASU 2017-11 is effective for public business entities for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2018. The adoption of ASU 2018-07 did not have a material impact on the Company’s consolidated financial statements.
Not yet adopted
ASU 2018-13 — Fair Value Measurement (Topic 820) - Disclosure Framework - Changes to the Disclosure Requirements for Fair Value Measurement
The amendments in this update are designed to improve the effectiveness of disclosures by removing, modifying and adding disclosures related to fair value measurements and is effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2019. The Company has not yet evaluated the impact of adoption of this ASU on its consolidated financial statements and related disclosures.
ASU 2018-18 — Collaborative Arrangements (Topic 808): Clarifying the Interaction between Topic 808 and Topic 606
The amendments in this update are intended to clarify the interaction between the accounting guidance for collaborative arrangements and revenue from contracts with customers. ASU 2018-18 is effective for public business entities for fiscal years beginning after December 15, 2019, including interim periods within that fiscal year. The Company has not yet evaluated the impact of adoption of this ASU on its consolidated financial statements and related disclosures.
81
ASU 2019-12 — Income Taxes (Topic 740)
The amendments in this update are intended to simplify the accounting for income taxes by eliminating certain exceptions related to the approach for intra-period tax allocation, the methodology for calculating income taxes in an interim period, and the recognition of deferred tax liabilities for outside basis differences. ASU 2019-12 also simplifies aspects of the accounting for franchise taxes and enacted changes in tax laws or rates. ASU 2019-12 is effective for fiscal years beginning after December 15, 2020, including interim periods within those fiscal years. Early adoption is permitted. Adoption of ASU 2019-12 requires certain changes to be made prospectively and other changes to be made retrospectively. The Company has not yet evaluated the impact of adoption of this ASU on its consolidated financial statements and related disclosures.
During the year ended June 30, 2020, other than ASU’s 2018-13, 2018-18 and 2019-12 there have been no new, or existing recently issued, accounting pronouncements that are of significance, or potential significance, that impact the Company’s consolidated financial statements.
|
3 |
Deferred costs |
The Company has incurred the following deferred costs at June 30, 2020. There were no deferred costs at June 30, 2019.
|
Description |
|
June 30, 2020 $ |
|
|
|
Deferred financing costs (note 11) |
|
|
84,944 |
|
|
Deferred loan costs (i) |
|
|
93,701 |
|
|
Balance - June 30, 2020 |
|
|
178,645 |
|
|
Short-term |
|
|
(93,701 |
) |
|
Long-term |
|
|
84,944 |
|
(i) Deferred loan costs include 125,000 share purchase warrants issued in respect of a loan issued to the Company by National Brain Tumor Society (“NBTS”) and the National Foundation for Cancer Research (“NFCR”) valued at $93,701 (“NBTS Warrants”) (Note 11). The NBTS Warrants are exercisable at a price of $1.09 per common share until June 19, 2025. The NBTS Warrants were valued on a Black-Scholes valuation with a risk-free interest rate of 0.37%, term of 5 years, volatility of 89.82% and a dividend rate of 0%. The estimated volatility of the Company’s common stock at the date of measurement is based on the historical volatility of the Company. The risk-free interest rate is based on rates published by the government for bonds with a maturity similar to the expected remaining life of the instrument at the valuation date. The expected term has been estimated using the remaining life of the warrant.
4 Related party transactions
Valent Technologies, LLC Agreements
One of the Company’s officers is a principal of Valent Technologies, LLC (“Valent”) and as result Valent is a related party to the Company.
On September 12, 2010, the Company entered into a Patent Assignment Agreement (the “Valent Assignment Agreement”) with Valent pursuant to which Valent transferred to the Company all its right, title and interest in and to the patents for VAL-083 owned by Valent. The Company now owns all rights and title to VAL-083 and is responsible for the drug’s further development and commercialization. In accordance with the terms of the Valent Assignment Agreement, Valent is entitled to receive a future royalty on all revenues derived from the development and commercialization of VAL-083. In the event that the Company terminates the agreement, the Company may be entitled to receive royalties from Valent’s subsequent development of VAL-083 depending on the development milestones the Company has achieved prior to the termination of the Valent Assignment Agreement.
On September 30, 2014, the Company entered into an exchange agreement (the “Valent Exchange Agreement”) with Valent and Del Mar (BC). Pursuant to the Valent Exchange Agreement, Valent exchanged its loan payable in the outstanding amount of $278,530 (including aggregate accrued interest to September 30, 2014 of $28,530), issued to Valent by Del Mar (BC), for 278,530 shares of the Company’s Series A Preferred Stock. The Series A Preferred Stock has a stated value of $1.00 per share (the “Series A Stated Value”) and is not convertible into common stock. The holder of the Series A Preferred Stock is entitled to dividends at the rate of 3% of the Series A Stated Value per year, payable quarterly in arrears. For the years ended June 30, 2020 and 2019 respectively, the Company recorded $8,356 related to the dividend paid to Valent. The dividends have been recorded as a direct increase in accumulated deficit.
82
Related party payables
At June 30, 2020 there is an aggregate amount of $663,865 (2019 - $325,208) payable to the Company’s officers and directors for fees, expenses, and accrued liabilities.
|
5 |
Derivative liabilities |
The Company has issued common stock purchase warrants. Based on the terms of certain of these warrants the Company determined that the warrants were derivative liabilities which are recognized at fair value at the date of the transaction and remeasured at fair value each reporting period with the changes in fair value recorded in the consolidated statement of operations. The estimated volatility of the Company’s common stock at the date of measurement is based on the historical volatility of the Company. The risk-free interest rate is based on rates published by the government for bonds with a maturity similar to the expected remaining life of the instrument at the valuation date. The expected life of the instrument has been estimated using the contractual life of the instrument.
2019 Investor Warrants
As part of the Company’s registered direct offering completed June 5, 2019 (note 6) the Company issued 760,500 share purchase warrants exercisable at a price of $3.10 until June 5, 2024 (the “2019 Investor Warrants”). The exercise price of the 2019 Investor Warrants is subject to adjustment in the event that the Company issues common stock at a price lower than the exercise price, subject to certain exceptions, prior to June 28, 2019. As a result, upon issuance on June 5, 2019, the Company has accounted for the 2019 Investor Warrants as a derivative liability. The change in fair value of the 2019 Investor Warrants from the date of issue until June 28, 2019 has been recorded in the consolidated statement of operations for the year ended June 30, 2019. Upon expiry of the repricing feature on June 28, 2019, the fair value of the derivative liability at that time of $492,884 was reclassified to equity.
2013 Investor Warrants
During the quarter ended March 31, 2013 the Company issued an aggregate of 328,125 units at a purchase price of $32.00 per unit, for aggregate gross proceeds of $10,500,000. Each unit consisted of one share of common stock and one five-year warrant (the “2013 Investor Warrants”) to purchase one share of common stock at an initial exercise price of $32.00. The exercise price of the 2013 Investor Warrants was subject to adjustment in the event that the Company issued common stock at a price lower than the exercise price, subject to certain exceptions. The 2013 Investor Warrants expired on March 31, 2019.
2015 Agent Warrants
As part of the Company’s financing completed in a prior period, the Company issued warrants to purchase 2,180 shares of common stock to certain placement agents (“2015 Agent Warrants”) and recognized them as a derivative liability of $29,594 at the time of issuance. The 2015 Agent Warrants are exercisable at a per share price equal to $30.00 until July 15, 2020 and expired unexercised subsequent to June 30, 2020 (note 11).
The Company’s derivative liabilities are summarized as follows:
|
Opening balance – June 30, 2018 |
|
|
1,117 |
|
|
Issuance of 2019 Investor Warrants |
|
|
925,270 |
|
|
Change in fair value of warrants |
|
|
(433,503 |
) |
|
Reclassification of 2019 Investor Warrants to equity |
|
|
(492,884 |
) |
|
Closing balance – June 30, 2019, and 2020 |
|
|
— |
|
At June 30, 2020, and 2019, the derivative liabilities consist of 2,180 2015 Agent warrants to purchase 2,180 shares of common stock.
83
|
6 |
Stockholders’ equity |
Preferred stock
Series B Preferred stock
|
|
|
Series B Preferred Stock |
|
|||||
|
|
|
Number of shares |
|
|
$ |
|
||
|
Balance – June 30, 2018 |
|
|
881,113 |
|
|
|
6,146,880 |
|
|
Conversion of Series B Preferred stock to common stock |
|
|
(207,500 |
) |
|
|
(1,447,576 |
) |
|
Balance – June 30, 2019 |
|
|
673,613 |
|
|
|
4,699,304 |
|
|
Conversion of Series B Preferred stock to common stock |
|
|
(25,000 |
) |
|
|
(174,407 |
) |
|
Balance – June 30, 2020 |
|
|
648,613 |
|
|
|
4,524,897 |
|
During the year ended June 30, 2016, the Company issued an aggregate of 902,238 shares of Series B Preferred Stock at a purchase price of $8.00 per share. Each share of Series B Preferred Stock is convertible into 0.25 shares of common stock equating to a conversion price of $32.00 (the “Conversion Price”) and will automatically convert to common stock at the earlier of 24 hours following regulatory approval of VAL-083 with a minimum closing bid price of $80.00, or five years from the respective final closing dates. The holders of the Series B Preferred Stock are entitled to an annual cumulative, in arrears, dividend at the rate of 9% payable quarterly. The 9% dividend accrues quarterly commencing on the date of issue and is payable quarterly on September 30, December 31, March 31, and June 30 of each year commencing on June 30, 2016. Dividends are payable solely by delivery of shares of common stock, in an amount for each holder equal to the aggregate dividend payable to such holder with respect to the shares of Series B Preferred Stock held by such holder divided by the Conversion Price. The Series B Preferred Stock does not contain any repricing features. Each share of Series B Preferred Stock entitles its holder to vote with the common stock on an as-converted basis.
The Series B Preferred Stock shall with respect to distributions of assets and rights upon the occurrence of a liquidation, rank (i) senior to the Company’s common stock and (ii) senior to the Special Voting Preferred Stock and (iii) senior to any other class or series of capital stock of the Company hereafter created which does not expressly rank pari passu with, or senior to, the Series B Preferred Stock. The Series B Preferred Stock shall be pari passu in liquidation to the Company’s Series A Preferred Stock. The liquidation value of the Series B Preferred Stock at June 30, 2020 is the stated value of $5,188,904.
In addition, the Company and the holders entered into a royalty agreement, pursuant to which the Company will pay the holders of the Series B Preferred Stock, in aggregate, a low, single-digit royalty based on their pro rata ownership of the Series B Preferred Stock on products sold directly by the Company or sold pursuant to a licensing or partnering arrangement (the “Royalty Agreement”).
Upon conversion of a holder’s Series B Preferred Stock to common stock, such holder shall no longer receive ongoing royalty payments under the Royalty Agreement but will be entitled to receive any residual royalty payments that have vested. Rights to the royalties shall vest during the first three years following the applicable closing date, in equal thirds to holders of the Series B Preferred Stock on each of the three vesting dates, upon which vesting dates such royalty amounts shall become vested royalties.
Pursuant to the Series B Preferred Stock dividend, during the year ended June 30, 2020, the Company issued 14,800 (2019 – 18,271) shares of common stock and recognized $8,616 (2019 – $80,431) as a direct increase in accumulated deficit. During the year ended June 30, 2020, a total of 25,000 (2019 – 207,500) shares of Series B Preferred Stock were converted for an aggregate 6,250 (2019 – 51,876) shares of common stock.
A total of 648,613 (2019 – 673,613) shares of Series B Preferred Stock are outstanding as of June 30, 2020, such that a total of 162,177 (2019 – 168,427) shares of common stock are issuable upon conversion of the Series B Preferred Stock as at June 30, 2020. Converted shares are rounded up to the nearest whole share.
Series A Preferred Stock
Effective September 30, 2014, the Company filed a Certificate of Designation of Series A Preferred Stock (the “Series A Certificate of Designation”) with the Secretary of State of Nevada. Pursuant to the Series A Certificate of Designation, the Company designated 278,530 shares of preferred stock as Series A Preferred Stock. The shares of Series A Preferred Stock have a stated value of $1.00 per share (the “Series A Stated Value”) and are not convertible into common stock. The holder of the Series A Preferred Stock is entitled to dividends at the rate of 3% of the Series A Stated Value per year, payable quarterly in arrears. Upon any liquidation of the Company, the holder of the Series A Preferred Stock will be entitled to be paid, out of any assets of the Company available for distribution to stockholders, the Series A Stated Value of the shares of Series A Preferred Stock held by such holder, plus any accrued but unpaid dividends thereon, prior to any payments being made with respect to the common stock. The Series A Preferred Stock is held by Valent (note 4).
84
The Series A Preferred Stock shall with respect to distributions of assets and rights upon the occurrence of a liquidation, rank (i) senior to the Company’s common stock, and (ii) senior to the Company’s Special Voting Preferred Stock and (iii) senior to any other class or series of capital stock of the Company hereafter created which does not expressly rank pari passu with, or senior to, the Series A Preferred Stock. The Series A Preferred Stock shall be pari passu in liquidation to the Company’s Series B Preferred Stock. The liquidation value of the Series A Preferred stock at June 30, 2020 of $278,530.
There was no change to the Series A Preferred stock for the years ended June 30, 2020 or 2019.
Special voting share
In connection with the Exchange Agreement (note 1), on the Reverse Acquisition Closing Date, the Company, Callco, Exchangeco and Computershare Trust Company of Canada (the “Trustee”) entered into a voting and exchange trust agreement (the “Trust Agreement”). Pursuant to the Trust Agreement, Company issued one share of Special Voting Preferred Stock (the “Special Voting Share”) to the Trustee, and the parties created a trust for the Trustee to hold the Special Voting Share for the benefit of the holders of the shares of Exchangeco acquired as part of the Reverse Acquisition (the “Exchangeable Shares”) (other than the Company and any affiliated companies) (the “Beneficiaries”). Pursuant to the Trust Agreement, the Beneficiaries will have voting rights in the Company equivalent to what they would have had they received shares of common stock in the same amount as the Exchangeable Shares held by the Beneficiaries.
In connection with the Exchange Agreement and the Trust Agreement, on January 17, 2013, the Company filed a certificate of designation of Special Voting Preferred Stock (the “Special Voting Certificate of Designation”) with the Secretary of State of Nevada. Pursuant to the Special Voting Certificate of Designation, one share of the Company’s blank check preferred stock was designated as Special Voting Preferred Stock. The Special Voting Preferred Stock votes as a single class with the common stock and is entitled to a number of votes equal to the number of Exchangeable Shares of Exchangeco outstanding as of the applicable record date (i) that are not owned by the Company or any affiliated companies and (ii) as to which the holder has received voting instructions from the holders of such Exchangeable Shares in accordance with the Trust Agreement.
The Special Voting Preferred Stock is not entitled to receive any dividends or to receive any assets of the Company upon any liquidation, and is not convertible into common stock of the Company.
The voting rights of the Special Voting Preferred Stock will terminate pursuant to and in accordance with the Trust Agreement. The Special Voting Preferred Stock was automatically cancelled during the year ended June 30, 2020 when the last Exchangeco share was exchanged for shares of Common Stock.
Common stock
Stock Issuances
Year ended June 30, 2020
Underwritten public offering
On August 16, 2019, the Company closed on the sale of (i) 4,895,000 shares of its common stock, par value $0.001 per share (the “Common Stock”), (ii) pre-funded warrants (“PFW”) to purchase an aggregate of 2,655,000 shares of Common Stock and (iii) common warrants to purchase an aggregate of 7,762,500 shares of Common Stock (“2020 Investor Warrants”), including 800,000 shares of Common Stock and 2020 Investor Warrants to purchase an aggregate of 1,012,500 shares of Common Stock sold pursuant to a partial exercise by the underwriters of the underwriters’ option to purchase additional securities, in the Company’s underwritten public offering (the “Offering”). Each share of Common Stock or PFW, as applicable, was sold together with a 2020 Investor Warrant to purchase one share of Common Stock at a combined effective price to the public of $1.00 per share of Common Stock and accompanying 2020 Investor Warrant.
The net proceeds from the Offering, including from the partial exercise of the underwriters’ option to purchase additional securities, were $6,582,966, after deducting underwriting discounts and commissions, and other offering expenses.
The 2020 Investor Warrants are exercisable at $1.00 per share until their expiry on August 16, 2024 and the PFW are exercisable at $0.01 per share at any time after August 16, 2019. The Company also issued 377,500 warrants to the underwriters of the Offering. The underwriter warrants are exercisable at $1.15 per share commencing February 10, 2020 until their expiry on August 14, 2022.
During the year ended June 30, 2020, all of the 2,655,000 PFW were exercised at $0.01 per PFW for proceeds of $26,550.
85
Year ended June 30, 2019
Public offering financing
On June 5, 2019 the Company completed a registered direct offering (the “2019 Registered Offering”) of an aggregate of 1,170,000 shares of common stock and warrants to purchase an additional 760,500 shares of common stock at a price of $3.10 per share and related warrant for gross proceeds of $3.6 million. The warrants have an exercise price of $3.10 per share, are immediately exercisable and have a term of exercise of five years (the “2019 Investor Warrants”).
The Company engaged a placement agent for the 2019 Registered Offering. Under the Company’s engagement agreement with the placement agent, the Company paid $290,160 in cash commission and other fees to the placement agent and issued warrants to purchase 46,800 shares of common stock to the placement agent (the “2019 Agent Warrants”). Commencing December 3, 2019, the 2019 Agent Warrants are exercisable at $3.875 per share until June 3, 2024.
In addition to the cash commission and other placement agent fees, the Company also incurred additional cash issue costs of $151,585 resulting in net cash proceeds of $3,185,255.
Shares issued for services
During the year ended June 30, 2020, the Company issued 22,520 (2019 – 3,444) shares of common stock for services resulting in the recognition of $13,396 (2019 – $13,777) in expense. All of the shares issued for services for the years ended June 30, 2020 and 2019 have been recognized as research and development expense.
2017 Omnibus Incentive Plan
As subsequently approved by the Company’s stockholders at an annual meeting of stockholders on April 11, 2018, the Company’s board of directors has approved adoption of the Company’s 2017 Omnibus Equity Incentive Plan (the “2017 Plan”). The board of directors also approved a form of Performance Stock Unit Award Agreement to be used in connection with grants of performance stock units (“PSUs”) under the 2017 Plan. Under the 2017 Plan, 2,280,000 shares of Company common stock are currently reserved for issuance, less the number of shares of common stock issued under the Del Mar (BC) 2013 Amended and Restated Stock Option Plan (the “Legacy Plan”) or that are subject to grants of stock options made, or that may be made, under the Legacy Plan. A total of 164,235 shares of common stock have been issued under the Legacy Plan and/or are subject to outstanding stock options granted under the Legacy Plan, and a total of 1,394,964 shares of common stock have been issued under the 2017 Plan and/or are subject to outstanding stock options granted under the 2017 Plan leaving 720,801 shares of common stock available at June 30, 2020 for issuance under the 2017 Plan if all such options under the Legacy Plan were exercised.
The maximum number of shares of Company common stock with respect to which any one participant may be granted awards during any calendar year is 8% of the Company’s fully diluted shares of common stock on the date of grant (excluding the number of shares of common stock issued under the 2017 Plan and/or the Legacy Plan or subject to outstanding awards granted under the 2017 Plan and/or the Legacy Plan). No award will be granted under the 2017 Plan on or after July 7, 2027, but awards granted prior to that date may extend beyond that date.
During the year ended June 30, 2020, the Company granted 1,041,016 stock options to officers and directors of the Company. Of the total stock options granted, 491,817 were granted under the previous 2017 Plan limit and 549,199 were granted subject to approval by the Company’s stockholders of the 2017 Plan share reserve increase. All of the stock options granted to officers and directors have an exercise price of $0.61 and expire on September 5, 2029. Of the 1,041,016 stock options granted, 375,000 vest pro rata monthly over one year from the date of grant and 666,016 vest as to one-sixth on the six-month anniversary of the grant date with the remaining five-sixths vesting pro rate monthly over 30 months commencing on the seven-month anniversary of the grant date. On June 26, 2020, the Company’s stockholders approved the increase in the number of shares available under the 2017 Plan to 2,280,000 and the 549,199 stock options were granted
In addition, during the year ended June 30, 2020, the Company granted 250,000 stock options to an officer of the Company, that were also approved by the Company’s stockholders on June 26, 2020. The options have an exercise price of $0.735 and expire November 12, 2029. The options vest upon the achievement of certain clinical development milestones.
At a special meeting of the Company’s stockholders held on August 14, 2020, the stockholders approved an increase in the total number of shares available under the 2017 Plan to 6,700,000.
86
Performance stock units
The Company’s board of directors granted PSUs under the 2017 Plan to the Company’s directors. The awards represent the right to receive shares of the Company’s common stock upon vesting of the PSU based on targets approved by the Company’s board of directors related to the Company’s fully diluted market capitalization. The PSUs vest at various fully diluted market capitalization levels with full vesting occurring upon the later of one year from the grant date and the Company achieving a fully diluted market capitalization of at least $500 million for five consecutive business days. On April 30, 2019 the Company’s directors all agreed to the cancellation of all PSUs. In relation to the PSU cancellation, the Company has recognized the full amount of the expense of the PSUs in the fourth quarter of fiscal 2019.
The following table sets forth changes in the PSUs outstanding under the 2017 Plan:
|
|
|
Number of PSUs outstanding |
|
|
|
Balance – June 30, 2018 |
|
|
120,000 |
|
|
Cancelled |
|
|
(120,000 |
) |
|
Balance – June 30, 2019 and 2020 |
|
|
— |
|
The Company has recognized $526,141 (including accelerated expense recognition due to the cancellation of the PSU’s of $322,877) in expense related to the PSUs during the year ended June 30, 2019 with all of it being recognized as general and administrative expense. There was no unrecognized PSU expense at June 30, 2019.
The PSUs were valued using the following assumptions:
|
|
|
June 30, 2019 |
|
|
|
Dividend rate |
|
|
0 |
% |
|
Volatility |
|
79.0 to 82.5% |
|
|
|
Risk-free rate |
|
2.56% to 2.71% |
|
|
|
Term – years |
|
1.67 to 3.24 |
|
|
Stock Options
The following table sets forth changes in stock options outstanding under all plans:
|
|
|
Number of stock options outstanding |
|
|
Weighted average exercise price |
|
||
|
Balance – June 30, 2018 |
|
|
262,683 |
|
|
|
24.27 |
|
|
Granted |
|
|
30,000 |
|
|
|
6.10 |
|
|
Forfeited |
|
|
(4,500 |
) |
|
|
28.37 |
|
|
Balance – June 30, 2019 |
|
|
288,183 |
|
|
|
22.31 |
|
|
Granted |
|
|
1,291,016 |
|
|
|
0.63 |
|
|
Forfeited |
|
|
(18,750 |
) |
|
|
0.61 |
|
|
Expired |
|
|
(1,250 |
) |
|
|
40.00 |
|
|
Balance – June 30, 2020 |
|
|
1,559,199 |
|
|
|
4.61 |
|
87
The following table summarizes stock options outstanding and exercisable under all plans at June 30, 2020:
|
Exercise price $ |
|
Number Outstanding at June 30, 2020 |
|
|
Weighted average remaining contractual life (years) |
|
|
Number exercisable at June 30, 2020 |
|
|||
|
0.61 |
|
|
1,022,266 |
|
|
|
9.18 |
|
|
|
447,756 |
|
|
0.74 |
|
|
250,000 |
|
|
|
9.37 |
|
|
|
— |
|
|
6.10 |
|
|
30,000 |
|
|
|
8.36 |
|
|
|
25,278 |
|
|
7.00 |
|
|
5,451 |
|
|
|
7.98 |
|
|
|
3,634 |
|
|
8.70 |
|
|
12,000 |
|
|
|
7.34 |
|
|
|
12,000 |
|
|
9.83 |
|
|
83,647 |
|
|
|
7.89 |
|
|
|
58,088 |
|
|
10.60 |
|
|
3,600 |
|
|
|
7.79 |
|
|
|
2,700 |
|
|
11.70 |
|
|
30,000 |
|
|
|
2.66 |
|
|
|
30,000 |
|
|
14.63 |
|
|
2,500 |
|
|
|
1.92 |
|
|
|
2,500 |
|
|
20.00 |
|
|
13,125 |
|
|
|
1.27 |
|
|
|
13,125 |
|
|
21.10 |
|
|
14,400 |
|
|
|
7.02 |
|
|
|
14,400 |
|
|
29.60 |
|
|
4,500 |
|
|
|
4.60 |
|
|
|
4,500 |
|
|
37.60 |
|
|
4,500 |
|
|
|
5.61 |
|
|
|
4,500 |
|
|
41.00 |
|
|
4,000 |
|
|
|
6.36 |
|
|
|
4,000 |
|
|
42.00 |
|
|
41,250 |
|
|
|
2.56 |
|
|
|
41,250 |
|
|
44.80 |
|
|
3,000 |
|
|
|
5.61 |
|
|
|
3,000 |
|
|
49.50 |
|
|
22,460 |
|
|
|
4.07 |
|
|
|
22,460 |
|
|
53.20 |
|
|
8,000 |
|
|
|
5.85 |
|
|
|
8,000 |
|
|
61.60 |
|
|
1,500 |
|
|
|
2.75 |
|
|
|
1,500 |
|
|
92.00 |
|
|
3,000 |
|
|
|
2.92 |
|
|
|
3,000 |
|
|
|
|
|
1,559,199 |
|
|
|
|
|
|
|
701,691 |
|
Included in the number of stock options outstanding are 2,500 stock options granted at an exercise price of CA$20.00. The exercise price of these options shown in the above table have been converted to US$14.63 using the period ending closing exchange rate. Stock options issued during the years ended June 30, 2020 and 2019 have been valued using a Black-Scholes pricing model with the following assumptions:
|
|
|
June 30, 2020 |
|
|
June 30, 2019 |
|
||
|
Dividend rate |
|
|
— |
% |
|
|
— |
% |
|
Volatility |
|
89% to 102% |
|
|
71% to 102% |
|
||
|
Risk-free rate |
|
0.32% to 1.50% |
|
|
1.62% to 3.17% |
|
||
|
Term – years |
|
4.7 to 5.7 |
|
|
0.1 to 3.0 |
|
||
The estimated volatility of the Company’s common stock at the date of issuance of the stock options is based on the historical volatility of the Company. The risk-free interest rate is based on rates published by the government for bonds with a maturity similar to the expected remaining life of the stock options at the valuation date.
The Company has recognized the following amounts as stock option expense for the periods noted:
|
|
|
Years ended June 30, |
|
|||||
|
|
|
2020 $ |
|
|
2019 $ |
|
||
|
Research and development |
|
|
86,835 |
|
|
|
74,667 |
|
|
General and administrative |
|
|
408,026 |
|
|
|
351,362 |
|
|
|
|
|
494,861 |
|
|
|
426,029 |
|
88
All of the stock option expense for the periods ended June 30, 2020 and 2019 has been recognized as additional paid in capital. The aggregate intrinsic value of stock options outstanding at June 30, 2020 was $79,554 (2019 - $0) and the aggregate intrinsic value of stock options exercisable at June 30, 2020 was $34,847 (2019 - $0). As of June 30, 2020, there was $177,442 in unrecognized compensation expense that will be recognized over the next 1.5 years. No stock options granted under the Company’s equity plans have been exercised during the year ended June 30, 2020. Upon the exercise of stock options new shares will be issued.
The following table sets forth changes in unvested stock options under all plans:
|
|
|
Number of options |
|
|
Weighted average exercise price $ |
|
|
Weighted average grant date fair value $ |
|
|||
|
Unvested at June 30, 2018 |
|
|
138,160 |
|
|
|
14.39 |
|
|
|
7.63 |
|
|
Granted |
|
|
30,000 |
|
|
|
6.10 |
|
|
|
2.56 |
|
|
Vested |
|
|
(83,170 |
) |
|
|
14.51 |
|
|
|
7.65 |
|
|
Unvested at June 30, 2019 |
|
|
84,990 |
|
|
|
11.35 |
|
|
|
5.82 |
|
|
Granted |
|
|
1,291,016 |
|
|
|
0.63 |
|
|
|
0.40 |
|
|
Vested |
|
|
(499,748 |
) |
|
|
1.87 |
|
|
|
1.12 |
|
|
Forfeited |
|
|
(18,750 |
) |
|
|
0.61 |
|
|
|
0.49 |
|
|
Unvested at June 30, 2020 |
|
|
857,508 |
|
|
|
0.98 |
|
|
|
0.52 |
|
The aggregate intrinsic value of unvested stock options at June 30, 2020 was $44,754 (2019 - $0). The unvested stock options have a remaining weighted average contractual term of 9.19 (2019 – 8.78) years.
Warrants
The following table sets forth changes in outstanding warrants:
|
|
|
Number of warrants |
|
|
Amount $ |
|
||
|
Balance – June 30, 2018 |
|
|
1,217,296 |
|
|
|
8,229,482 |
|
|
Exercise and exchange of 2018 Investor Warrants (i) |
|
|
(495,000 |
) |
|
|
(2,210,697 |
) |
|
Issuance of 2019 Investor Warrants (note 5) |
|
|
760,500 |
|
|
|
492,884 |
|
|
Issuance of 2019 Agent Warrants (iv) |
|
|
46,800 |
|
|
|
52,899 |
|
|
Warrants issued for services (iii) |
|
|
14,000 |
|
|
|
23,715 |
|
|
Balance – June 30, 2019 |
|
|
1,543,596 |
|
|
|
6,588,283 |
|
|
Underwritten public offering |
|
|
10,417,500 |
|
|
|
3,924,384 |
|
|
Issuance of 2020 Underwriter Warrants |
|
|
377,500 |
|
|
|
164,436 |
|
|
Exercise of PFW |
|
|
(2,655,000 |
) |
|
|
(2,397,935 |
) |
|
Exercise of 2020 Investor Warrants (ii) |
|
|
(25,000 |
) |
|
|
(12,138 |
) |
|
Warrants issued for services (iii) |
|
|
655,000 |
|
|
|
287,183 |
|
|
Expiry of warrants issued for services (iii) |
|
|
(4,140 |
) |
|
|
(29,877 |
) |
|
Balance – June 30, 2020 |
|
|
10,309,456 |
|
|
|
8,524,336 |
|
|
i) |
On November 25, 2018, the Company entered into Warrant Exercise and Exchange Agreements (the “Warrant Exercise Agreements”) with certain holders (the “Exercising Holders”) of the 2018 Investor Warrants. Pursuant to the Warrant Exercise Agreements, in order to induce the Exercising Holders to exercise the 2018 Investor Warrants for cash, the Company agreed to reduce the exercise price from $12.50 to $4.00 per share. Pursuant to the Warrant Exercise Agreements, the Exercising Holders exercised their 2018 Investor Warrants with respect to an aggregate of 197,500 shares of common stock underlying such 2018 Investor Warrants (the “Exercised Shares”). The Company received net proceeds of $720,165, comprising aggregate gross proceeds of $790,000 net of expenses of $69,835, from the exercise of the 2018 Investor Warrants. |
89
|
ii) |
A total of 25,000 2020 Investor Warrants were exercised at $1.00. |
|
iii) |
Warrants issued for services are exercisable at various prices and expire at the various dates noted in the table below. |
|
iv) |
As part of the financing completed by the Company on June 5, 2019, the Company issued the 2019 Agent Warrants. Commencing December 3, 2019, the 2019 Agent Warrants are exercisable at $3.875 until June 3, 2024. |
The following table summarizes the Company’s outstanding warrants as of June 30, 2020:
|
Description of warrants |
|
Number |
|
|
Exercise price $ |
|
|
Expiry date |
||
|
2020 Investor warrants |
|
|
7,737,500 |
|
|
|
1.00 |
|
|
August 16, 2024 |
|
2019 Investor warrants |
|
|
760,500 |
|
|
|
3.10 |
|
|
June 5, 2024 |
|
2019 Investor warrants |
|
|
280,000 |
|
|
|
12.50 |
|
|
September 22, 2022 |
|
2017 Investor warrants |
|
|
207,721 |
|
|
|
35.00 |
|
|
April 19, 2022 |
|
2015 Investor warrants |
|
|
97,905 |
|
|
|
30.00 |
|
|
July 31, 2020 (i) |
|
NBTS Warrants |
|
|
125,000 |
|
|
|
1.09 |
|
|
June 19, 2025 (ii) |
|
Warrants issued for services |
|
|
250,000 |
|
|
|
0.64 |
|
|
January 20, 2024 |
|
Warrants issued for services |
|
|
280,000 |
|
|
|
0.75 |
|
|
November 18, 2023 |
|
Warrants issued for services |
|
|
26,500 |
|
|
|
30.00 |
|
|
July 1, 2020 to February 1,2021 (iii) |
|
Warrants issued for services |
|
|
6,000 |
|
|
|
17.80 |
|
|
January 25, 2023 |
|
Warrants issued for services |
|
|
33,600 |
|
|
|
11.70 |
|
|
February 27, 2023 |
|
Warrants issued for services |
|
|
12,000 |
|
|
|
9.00 |
|
|
September 15, 2023 |
|
Warrants issued for services |
|
|
2,000 |
|
|
|
9.00 |
|
|
October 11, 2021 |
|
2020 Underwriter Warrants |
|
|
377,500 |
|
|
|
1.15 |
|
|
August 14, 2022 |
|
2019 Agent warrants |
|
|
46,800 |
|
|
|
3.875 |
|
|
June 3, 2024 |
|
2019 Agent warrants |
|
|
40,000 |
|
|
|
12.50 |
|
|
September 20, 2022 |
|
2017 Agent warrants |
|
|
13,848 |
|
|
|
40.60 |
|
|
April 12, 2022 |
|
2016 Agent warrants |
|
|
10,402 |
|
|
|
40.00 |
|
|
May 12, 2021 |
|
2015 Agent warrants |
|
|
2,180 |
|
|
|
30.00 |
|
|
July 15, 2020 (i) |
|
|
|
|
10,309,456 |
|
|
|
|
|
|
|
|
(i) |
Expired unexercised subsequent to June 30, 2020. |
|
(ii) |
NBTS Warrants issued with respect to loan proceeds received subsequent to June 30, 2020 (notes 3 and 11). |
|
(iii) |
1,500 warrants issued for services expired unexercised subsequent to June 30, 2020. |
|
7 |
Income taxes |
For the years ended June 30, 2020, and 2019, the Company did not record a provision for income taxes due to a full valuation allowance against our deferred tax assets.
90
Significant components of the Company’s deferred tax assets and deferred tax liabilities are shown below:
|
|
|
June 30, 2020 $ |
|
|
June 30, 2019 $ |
|
||
|
Deferred tax assets: |
|
|
|
|
|
|
|
|
|
Non-capital losses carried forward |
|
|
11,870,922 |
|
|
|
10,823,529 |
|
|
Capital losses carried forward |
|
|
17,925 |
|
|
|
17,925 |
|
|
Financing costs |
|
|
221,276 |
|
|
|
— |
|
|
Scientific research and development |
|
|
604,489 |
|
|
|
534,398 |
|
|
Scientific research and development – Investment Tax Credits (“ITC”) |
|
|
534,355 |
|
|
|
484,135 |
|
|
|
|
|
13,248,967 |
|
|
|
11,859,987 |
|
|
Deferred tax liabilities: |
|
|
|
|
|
|
|
|
|
Scientific research and development – ITC |
|
|
(88,929 |
) |
|
|
(81,386 |
) |
|
|
|
|
13,160,038 |
|
|
|
11,778,601 |
|
|
Valuation allowance |
|
|
(13,160,038 |
) |
|
|
(11,778,601 |
) |
|
Net future tax assets |
|
|
— |
|
|
|
— |
|
The income tax benefit of these tax attributes has not been recorded in these consolidated financial statements because of the uncertainty of their recovery. The Company’s effective income tax rate differs from the statutory income tax rate of 21% (2019 – 21%).
The differences arise from the following items:
|
|
|
June 30, 2020 $ |
|
|
June 30, 2019 $ |
|
||
|
Tax recovery at statutory income tax rates |
|
|
(1,916,442 |
) |
|
|
(1,690,126 |
) |
|
Permanent differences |
|
|
142,523 |
|
|
|
(527,532 |
) |
|
Effect of rate differentials between jurisdictions |
|
|
(239,465 |
) |
|
|
(429,531 |
) |
|
Effect of foreign exchange rates |
|
|
347,510 |
|
|
- |
|
|
|
Scientific research and development – ITC |
|
|
(38,252 |
) |
|
|
(39,807 |
) |
|
Other |
|
|
322,689 |
|
|
|
106,320 |
|
|
Change in valuation allowance |
|
|
1,381,437 |
|
|
|
2,580,676 |
|
|
|
|
|
— |
|
|
|
— |
|
The Company has no current income tax expense for the year ended June 30, 2020, as there was a taxable loss for this period. The components of the Company’s loss before income taxes for the year ended June 30, 2020 were allocated as to $5.2 million in the US and $4.0 million in Canada. As of June 30, 2020, the Company had combined US and Canadian net operating loss carry forwards of $47.8 million (2019 – $43.2 million). The U.S. federal NOL carryforwards consist of $10.5 million generated before July 1, 2018, which begin expiring in 2030, and $6.7 million that can be carried forward indefinitely, but are subject to the 80% taxable income limitation. The Canadian NOL carryforwards of $30.6 million begin expiring in 2030. In addition, the Company has non-refundable Canadian federal investment tax credits of $329,368 (2019 - $303,969) that expire between 2029 and 2040 and non-refundable British Columbia investment tax credits of $204,987 (2019 – $166,000) that expire between 2020 and 2030. The Company also has Canadian scientific research and development tax incentives of $2.2 million (2019 – $2.0 million) that do not expire.
We file U.S., U.S. state and Canadian income tax returns with varying statues of limitations. The tax years from 2010 to 2020 remain open to examination due to the carryover of unused NOL carryforwards and tax credits.
Internal Revenue Code (“IRC”) Section 382 and 383 places a limitation on the amount of taxable income that can be offset by NOL and credit carryforwards after a change in control (generally greater than 50% change in ownership within a three-year period) of a loss corporation. Generally, after a change in control, a loss corporation cannot deduct NOL and credit carryforwards in excess of the IRC Section 382 and 383 limitation. The limitation in the federal and state NOL and research and development credit carryforwards reduce the deferred tax assets, which are further offset by a full valuation allowance. The limitation can result in the expiration of the NOLs and research and development credit carryforwards available. We have performed an IRC Section 382 and 383 analysis and determined there was an ownership change in 2013. The Company has not performed any section 382 and 383 analysis since 2013. An assessed change in ownership subsequent to 2013 could limit future use of NOL and research and development credit carryforwards.
91
|
8 |
Commitments and contingencies |
The Company has the following obligations over the next five fiscal years ending June 30, 2025:
Clinical development
The Company has entered into contracts for drug manufacturing, clinical study management and safety related to its Phase II clinical trials, and a one-year loan (note 11) for a total of $1,419,520. Pursuant to the commitment for clinical trial management, the Company has paid a total of $41,938 in deposits related to study initiation and certain study costs. These deposits are available to be applied against invoices received from the contract research organization but have not been netted against the Company’s commitments for the fiscal year ended June 30, 2020.
Office lease
The Company currently rents its shared head office on a one-year renewable lease at $189 per month. The Company also rents its administrative offices on a month-to-month basis at a rate of $3,187 (CA$4,357) per month. During the year ended June 30, 2020, the Company recorded a total of $40,130 as rent expense (2019 - $52,926).
|
9 |
Supplementary statement of cash flows information |
|
|
|
Year ended June 30, 2020 |
|
|
Year ended June 30, 2019 |
|
||
|
Series B Preferred Stock common stock dividend (note 6) |
|
|
8,616 |
|
|
|
80,431 |
|
|
Non-cash issue costs (note 6) |
|
|
182,257 |
|
|
|
52,899 |
|
|
Issue costs in accounts payable (note 6) |
|
|
— |
|
|
|
64,432 |
|
|
Deferred costs in accounts payable (note 3) |
|
|
59,944 |
|
|
|
— |
|
|
Warrants issued as deferred costs (notes 3 and 11) |
|
|
93,701 |
|
|
|
— |
|
|
Reclassification of derivative liability to equity (note 5) |
|
|
— |
|
|
|
492,884 |
|
|
Conversion of Series B Preferred Stock to common stock (note 6) |
|
|
174,407 |
|
|
|
1,447,576 |
|
|
Income taxes paid |
|
|
— |
|
|
|
— |
|
|
Interest paid |
|
|
— |
|
|
|
— |
|
|
10 |
Financial risk management |
Market risk
Market risk is the risk that changes in market prices, such as foreign exchange rates, interest rates and equity prices will affect the Company’s income or valuation of its financial instruments.
The Company is exposed to financial risk related to fluctuation of foreign exchange rates. Foreign currency risk is limited to the portion of the Company’s business transactions denominated in currencies other than the United Sates dollar, primarily general and administrative expenses incurred in Canadian dollars. The Company believes that the results of operations, financial position and cash flows would be affected by a sudden change in foreign exchange rates but would not impair or enhance its ability to pay its Canadian dollar accounts payable. The Company manages foreign exchange risk by converting its US$ to CA$ as needed. The Company maintains the majority of its cash in US$. As at June 30, 2020, Canadian dollar denominated accounts payable and accrued liabilities exposure in US$ totaled $152,347.
|
a) |
Foreign exchange risk |
Foreign exchange risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in foreign exchange rates. If foreign exchange rates were to fluctuate within +/-10% of the closing rate at year-end, the maximum exposure is $17,853.
92
Balances in foreign currencies at June 30, 2020 and 2019 are as follows:
|
|
|
June 30, 2020 balances CA$ |
|
|
June 30, 2019 balances CA$ |
|
||
|
Trade payables |
|
|
167,499 |
|
|
|
201,279 |
|
|
Cash |
|
|
20,981 |
|
|
|
24,248 |
|
|
Interest, taxes, and other receivables |
|
|
12,808 |
|
|
|
26,099 |
|
|
b) |
Interest rate risk |
The Company is subject to interest rate risk on its cash and cash equivalents and believes that the results of operations, financial position and cash flows would not be significantly affected by a sudden change in market interest rates relative to the investment interest rates due to the short-term nature of the investments. As at June 30, 2020, cash and cash equivalents held by the Company were $2,392,402. The Company’s cash balance currently earns interest at standard bank rates. If interest rates were to fluctuate within +/-10% of the closing rate at year end the impact of the Company’s interest-bearing accounts will be not be significant due to the current low market interest rates.
The only financial instruments that expose the Company to interest rate risk are its cash and cash equivalents.
Liquidity risk
Liquidity risk is the risk that the Company will encounter difficulty in raising funds to meet cash flow requirements associated with financial instruments. The Company continues to manage its liquidity risk based on the outflows experienced for the period ended June 30, 2020 and is undertaking efforts to conserve cash resources wherever possible. The maximum exposure of the Company’s liquidity risk is $2,674,923 as at June 30, 2020.
Credit risk
Credit risk arises from cash and cash equivalents, deposits with banks, financial institutions, and contractors as well as outstanding receivables. The Company limits its exposure to credit risk, with respect to cash and cash equivalents, by placing them with high quality credit financial institutions. The Company’s cash equivalents consist primarily of operating funds with commercial banks. Of the amounts with financial institutions on deposit, the following table summarizes the amounts at risk should the financial institutions with which the deposits are held cease trading:
The maximum exposure of the Company’s credit risk is $9,401 at June 30, 2020 relating to interest, taxes, and other receivables. The credit risk related to uninsured cash and cash equivalents balances is $2,232,270 at June 30, 2020.
|
|
|
Cash and cash equivalents $ |
|
|
Insured amount $ |
|
|
Non- insured amount $ |
|
|||
|
|
|
|
2,392,402 |
|
|
|
160,132 |
|
|
|
2,232,270 |
|
Concentration of credit risk
Financial instruments that subject the Company to credit risk consist primarily of cash and cash equivalents.
The Company places its cash and cash equivalents in accredited financial institutions and therefore the Company’s management believes these funds are subject to minimal credit risk. The Company has no significant off-balance sheet concentrations of credit risk such as foreign currency exchange contracts, option contracts or other hedging arrangements.
|
11 |
Subsequent events |
The Company has evaluated its subsequent events from June 30, 2020 through the date these consolidated financial statements were issued and has determined that there are no subsequent events requiring disclosure in these consolidated financial statements other than the items noted below.
93
Adgero merger
On June 9, 2020, the Company, Adgero Acquisition Corp., a wholly-owned subsidiary of the Company (“Merger Sub”), and Adgero, entered into an Agreement and Plan of Merger and Reorganization (the “Merger Agreement”) pursuant to which Merger Sub will merge with and into Adgero, with Adgero surviving the merger and becoming a direct, wholly-owned subsidiary of the Company (the “Merger”).
Subject to the terms and conditions of the Merger Agreement, at the effective time of the Merger (the “Effective Time”), (i) each outstanding share of Adgero common stock (the “Adgero Common Stock”) (other than any shares held as treasury stock that will be cancelled) was converted into shares of Company common stock (the “Kintara Common Stock”) based on the exchange ratio, (ii) each outstanding warrant to purchase Adgero Common Stock was converted into a warrant exercisable for that number of shares of Kintara Common Stock equal to the product of (x) the aggregate number of shares of Adgero Common Stock for which such warrant was exercisable and (y) the Exchange Ratio (as defined in the Merger Agreement); and (iii) each outstanding Adgero stock option, whether vested or unvested, that had not been exercised was cancelled for no consideration. On August 19, 2020, upon the terms and subject to the conditions set forth in the Merger Agreement, Merger Sub merged with and into Adgero, the separate corporate existence of Merger Sub ceased and Adgero continued its existence under Delaware law as the surviving corporation and a direct, wholly-owned subsidiary of the Company.
The Exchange Ratio in the Merger Agreement was negotiated so that the existing stockholders of Adgero would own 49.5% of the total voting shares outstanding of the Company and the existing stockholders of the Company would own 50.5% of the total voting shares outstanding of the Company immediately after the merger (less the effect of the payment of cash in lieu of any fraction share of Kintara Common Stock). The final Exchange Ratio determined immediately prior to the Effective Time to reflect the Company’s and Adgero’s capitalization as of immediately prior to such time was 1.574.
Upon closing of the Merger, the Company issued 11,439,013 shares of Kintara Common Stock and 2,313,908 stock purchase warrants to the security holders of Adgero. The warrants issued to the Adgero warrant holders are exercisable at $3.18 per share. Upon closing of the Merger, the Company issued 571,951 shares of Kintara Common Stock to the placement agent as a success fee.
In connection with the Merger, the Company completed a private placement of Series C Convertible Preferred Stock (the “Series C Stock”) in three separate closings. Each share of Series C Stock was issued at a purchase price of $1,000 per share and is convertible into shares of Kintara Common Stock based on the respective conversion price which was determined at the closing of each round of the private placement. The Series C Stock is entitled to receive dividends, payable in shares of Kintara Common Stock at a rate of 10%, 15%, 20% and 25% of the number of shares of Kintara Common Stock issuable upon conversion of the Series C Stock, on the 12th, 24th, 36th and 48th month, anniversary of the initial closing of the private placement which occurred on August 19, 2020. In addition, the Company issued warrants to the placement agent equal to 10% of the number of shares of Series C Stock issued in the private placement. As of June 30, 2020, the Company had incurred deferred financing costs of $84,944 with respect to the private placement (note 3).
As result of the three separate closings of the private placement, the Company issued a total of 25,028 Series C Stock at a purchase price of $1,000 per share for total gross proceeds of approximately $25 million, or net proceeds of approximately $21.7 million. The conversion prices for the Series C-1 Preferred Stock, Series C-2 Preferred Stock and Series C-3 Preferred Stock are $1.16, $1.214 and $1.15, respectively. Based on the conversion prices of the three respective classes of Series C Stock, the 25,028 shares of Series C Stock will be convertible into an aggregate of 21,516,484 shares of Kintara Common Stock. In addition, the Company issued warrants to purchase 2,504 shares of Series C Stock to the placement agent.
The Merger is expected to be accounted for as an acquisition of the net assets of Adgero as Adgero does not constitute a business. As at June 30, 2020, the Company had incurred costs of $1,053,697 with respect to the Merger. These costs have been expensed as of June 30, 2020.
Loan from National Brain Tumor Society and National Foundation for Cancer Research
Subsequent to June 30, 2020, the Company received proceeds of $500,000 from NBTS and NFCR to support VAL-083's preparation for participation in the Global Coalition for Adaptive Research's (“GCAR”) sponsored trial, Glioblastoma (GBM) Adaptive Global Innovative Learning Environment (GBM AGILE) study (“NBTS Loan”). The Company issued 125,000 NBTS Warrants which are exercisable at a price of $1.09 per common share until June 19, 2025 and have been included in deferred financing costs as at June 30, 2020 (note 3). The NBTS Loan is secured by a promissory note, accrues interest at a rate of 6% per annum and matures on June 19, 2021.
94
Warrants
Subsequent to June 30, 2020, 363,623 warrants were exercised at $1.00 per share.
Stock Options
Subsequent to June 30, 2020, a total of 222,887 stock options issued to directors of the Company were amended such that the period to exercise vested stock options from the date of termination with the Company was extended from 90 days to one year. Of the total of 222,887, 66,850 had their expiry increased from September 26, 2020 to June 26, 2021 and 156,037 had their expiry increased from November 19, 2020 to August 19, 2021. In addition, 14,014 stock options were forfeited.
On September 15, 2020, a total of 4,698,687 stock options were issued to executive officers and directors of the Company, all with an exercise price of $1.70 per share. Of the total granted, 4,218,687 stock options vest as to 1/6 on March 15, 2021 with the remaining portion of the 4,218,687 vesting in equal monthly installments over a period of 30 months commencing on April 15, 2021. In addition, of the total stock options granted, 480,000 vest in 12 equal monthly installments beginning on October 15, 2020. All of the stock options granted have a 10-year term and are subject to cancellation upon the grantees’ termination of service for the Company, with certain exceptions.
95
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in the reports that we file or submit under the Exchange Act, is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and our Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure.
Under the supervision and with the participation of our management, including our Chief Executive Officer and our Chief Financial Officer, we have evaluated the effectiveness of our disclosure controls and procedures as of June 30, 2020. Based on that evaluation, our Chief Executive Officer and our Chief Financial Officer concluded that, for the reasons set forth below, our disclosure controls and procedures were not effective as of June 30, 2020.
Internal Control Over Financial Reporting
Management’s Annual Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Internal control over financial reporting is a process designed by, or under the supervision of, our Chief Executive Officer and our Chief Financial Officer and effected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Internal control over financial reporting includes policies and procedures that (i) pertain to the maintenance of records that in reasonable detail accurately and fairly reflect our transactions and dispositions of our assets; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures of the are being made only in accordance with authorizations of our management and directors; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on the financial statements.
Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework provided in Internal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based upon the evaluation, our management concluded that our internal control over financial reporting was not effective as of June 30, 2020 because of material weaknesses in our internal control over financial reporting. A material weakness is a control deficiency or combination of deficiencies in internal control, such that there is a reasonable possibility that a material misstatement of the entity’s financial statements will not be prevented or detected and corrected on a timely basis. Our management concluded that we have a material weakness in the design and operating effectiveness of our internal controls over financial reporting because of inadequate segregation of duties over authorization, review and recording of transactions, as well as the financial reporting of such transactions.
Remediation Plan for the Material Weakness
Management has been actively engaged in developing remediation plans to address the above material weakness. The remediation efforts in process or expected to be implemented include the following:
|
|
• |
Management has engaged an external consulting firm to assist with our internal accounting functions and further enhance our internal controls which has increased the number of personnel involved in financial reporting. |
|
|
• |
Over the course of the fiscal year ended June 30, 2020, we have continued to integrate personnel from our external consulting firm into our systems of internal controls in the following areas: |
|
|
o |
Preparation and review of accounting and financial documents; and |
|
|
o |
Payment processing procedures. |
96
Despite the existence of this material weakness, we believe the financial information presented herein is materially correct and in accordance with generally accepted accounting principles in the United States.
While the implementation of improved controls and procedures has strengthened our internal control framework and disclosure controls, we continue to believe we have a material weakness related to the lack of sufficient segregation of duties.
This Annual Report does not include an attestation report of our registered public accounting firm regarding internal control over financial reporting. Management’s report is not subject to attestation by our registered public accounting firm because we are not an accelerated filer under the Exchange Act.
Changes in Control Over Financial Reporting
During the fourth quarter of the year ended June 30, 2020, there was no change in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f)) under the Exchange Act) that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting
As we continue to evaluate and work to improve our internal control over financial reporting, we may determine to take additional measures to address the material weakness or determine to supplement or modify certain of the remediation measures described above.
On September 15, 2020, a total of 4,698,687 stock options were issued to executive officers and directors of the Company, all with an exercise price of $1.70 per share. Specifically, the Board approved a grant of 2,715,004 stock options to Saiid Zarrabian, the Company’s President and Chief Executive Officer. The first 1/6 of the grant, or 452,501 of the stock options vest on March 15, 2021 with the remaining stock options vesting in equal monthly installments over a period of 30 months commencing on April 15, 2021. The Board also approved grants of 606,557 stock options, 87,437 stock options, 506,647 stock options and 303,041 stock options to Scott Praill, the Company’s Chief Financial Officer, to Dennis Brown, the Company’s Chief Scientific Officer, to John Liatos, the Company’s Senior Vice President, Business Development, and to Steve Rychnovsky, the Company’s Vice President, Research and Development, respectively. Such stock options have the same vesting schedule as the stock options granted to Mr. Zarrabian. In addition, the Board approved a grant of 120,000 stock options to each of the Company’s four non-employee directors. The stock options granted to the directors vest in 12 equal monthly installments beginning on October 15, 2020.
All of the stock options approved by the Board have a 10-year term and are subject to cancellation upon the grantees’ termination of service for the Company, with certain exceptions.
97
Item 10. Directors, Executive Officers and Corporate Governance.
Below are the names and certain information regarding our executive officers and directors.
|
Name |
|
Age |
|
Position |
|
Robert E. Hoffman |
|
54 |
|
Chairman of the Board |
|
Saiid Zarrabian |
|
67 |
|
President, Chief Executive Officer and Director |
|
Dennis Brown, PhD |
|
71 |
|
Chief Scientific Officer |
|
Scott Praill, CPA |
|
54 |
|
Chief Financial Officer |
|
John Liatos |
|
52 |
|
Senior Vice President, Business Development, Director |
|
Steven Rychnovsky, PhD |
|
61 |
|
Vice President, Research and Development |
|
Robert J. Toth, Jr., MBA |
|
56 |
|
Director |
|
Laura Johnson |
|
55 |
|
Director |
|
Keith Murphy |
|
48 |
|
Director |
Robert E. Hoffman has served as a director of Kintara since April 11, 2018 and as our Chairman since June 2, 2018. He has served as a member of Kura Oncology, Inc.’s board of directors since March 2015 and as a member of Aslan Pharmaceuticals, Inc.’s board of directors since October 30, 2018. Mr. Hoffman has served as Senior Vice President and Chief Financial Officer of Heron Therapeutics, Inc., a publicly-held pharmaceutical company since April 2017. Prior to joining Heron Therapeutics, Inc., Mr. Hoffman served as Executive Vice President and Chief Financial Officer of Innovus Pharmaceuticals, Inc., a publicly-held pharmaceutical company, from September 2016 to April 2017. From July 2015 to September 2016, Mr. Hoffman served as Chief Financial Officer of AnaptysBio, Inc., a publicly-held biotechnology company. From June 2012 to July 2015, Mr. Hoffman served as the Senior Vice President, Finance and Chief Financial Officer of Arena Pharmaceuticals, Inc., or Arena, a publicly-held biopharmaceutical company. From August 2011 to June 2012 and previously from December 2005 to March 2011, he served as Arena’s Vice President, Finance and Chief Financial Officer and in a number of various roles of increasing responsibility from 1997 to December 2005. From March 2011 to August 2011, Mr. Hoffman served as Chief Financial Officer for Polaris Group, a biopharmaceutical drug company. Mr. Hoffman formerly served as a member of the board of directors of CombiMatrix Corporation, a molecular diagnostics company, MabVax Therapeutics Holdings, Inc., a biopharmaceutical company and Aravive, Inc., a clinical stage biotechnology company, from October 2018 to April 2020. Mr. Hoffman serves as a member of the Financial Accounting Standards Board’s Small Business Advisory Committee and the steering committee of the Association of Bioscience Financial Officers. Mr. Hoffman formerly served as a director and President, of the San Diego Chapter of Financial Executives International. Mr. Hoffman holds a B.B.A. from St. Bonaventure University, and is licensed as a C.P.A. (inactive) in the State of California. Mr. Hoffman’s financial and executive business experience qualifies him to serve on our board of directors.
Saiid Zarrabian has served as a director of Kintara since July 7, 2017, Chief Executive Officer since November 3, 2017, and President since January 1, 2018. From 2014 to 2015 he operated a private personal business. Since October 2016, Mr. Zarrabian has served as an advisor to Redline Capital Partners, S.A., a Luxembourg based investment firm. From 2012 to 2014 he served as Chairman and member of the board of directors of La Jolla Pharmaceutical Company during which time the company transitioned from an OTC listed company to a NASDAQ listed company. From 2012 to 2013 he served as President of the Protein Production Division of Intrexon Corporation, a synthetic biology company. He has also previously served as CEO and member of the board of directors of Cyntellect, Inc., a stem cell processing and visualization Instrumentation company until its sale in 2012, as President and COO of Senomyx, Inc., a company focused on discovery and commercialization of new flavor ingredients, and as COO of Pharmacopeia, Inc., a former publicly-traded provider of combinatorial chemistry discovery services and compounds, where he also served as President & COO of its MSI Division. In addition, Mr. Zarrabian has served on numerous private and public company boards, including at Immune Therapeutics, Inc., Exemplar Pharma, LLC, Ambit Biosciences Corporation, eMolecules, Inc., and Penwest Pharmaceuticals CO. His other experience includes COO at Molecular Simulations, COO of Symbolics, Inc., and as R&D Director at Computervision, Inc. Mr. Zarrabian’s business executive knowledge and experience qualify him to serve on our board of directors.
Dennis Brown, PhD, has served as Kintara’s chief scientific officer since January 25, 2013. He also served as a director of DelMar from February 11, 2013 to April 11, 2018. Dr. Brown is one of our founders and has served as Chief Scientific Officer and director of Del Mar (BC) since inception. Dr. Brown has more than thirty years of drug discovery and development experience. He has served as Chairman of Mountain View Pharmaceutical’s board of directors since 2000 and is the President of Valent. In 1999 he founded ChemGenex Therapeutics, which merged with a publicly traded Australian company in 2004 to become ChemGenex Pharmaceuticals (ASX: CXS/NASDAQ: CXSP), of which he served as President and a Director until 2009. He was previously a co-founder of Matrix Pharmaceutical, Inc., where he served as Vice President (VP) of Scientific Affairs from 1985-1995 and as VP, Discovery Research, from 1995-1999. He also previously served as an Assistant Professor of Radiology at Harvard University Medical School and as a Research Associate in Radiology at Stanford University Medical School. He received his B.A. in Biology and Chemistry (1971), M.S. in Cell Biology (1975) and Ph.D. in Radiation and Cancer Biology (1979), all from New York University. Dr. Brown is an inventor of many issued U.S. patents and applications, many with foreign counterparts.
98
Scott Praill, CPA, BSc. has served as our chief financial officer since January 29, 2013 and previously served as a consultant to Del Mar (BC). From 2004 to 2012 Mr. Praill was an independent consultant providing accounting and administrative services to companies in the resource industry. Mr. Praill served as CFO of Strata Oil & Gas, Inc. from June 2007 to September 2008. From November 1999 to October 2003 Mr. Praill was Director of Finance at Inflazyme Pharmaceuticals Inc. Mr. Praill completed his articling at Price Waterhouse (now PricewaterhouseCoopers LLP) and obtained his Chartered Professional Accountant designation in 1996. Mr. Praill obtained his Certified Public Accountant (Illinois) designation in 2001. Mr. Praill received a Financial Management Diploma (Honors), from British Columbia Institute of Technology in 1993, and a Bachelor of Science from Simon Fraser University in 1989.
John Liatos has served as senior vice president, business development and as a director of Kintara since August 19, 2020. He previously served as Adgero’s interim Chief Executive Officer since April 2018, Chief Financial Officer since October, 2017 and a director of Adgero since April 2020. Mr. Liatos has over 20 years of financial and operational experience in the private equity and venture capital industries. Since 2008, Mr. Liatos has served as Co-Founding Partner at Aceras BioMedical, LLC, an investment vehicle focused on forming and managing new companies to acquire and develop pre-commercial stage biomedical assets. While at Aceras BioMedical, LLC, Mr. Liatos was involved in the overall formation and business strategy of the Aceras BioMedical, LLC portfolio companies, including functioning as interim Chief Financial Officer and Chief Operations Officer through the first twelve to eighteen months of operations for such portfolio companies. From 2005 to 2008, Mr. Liatos served as Chief Financial Officer to Paramount Biosciences, LLC, a drug development and biotechnology investment firm. From 1997 to 2005, Mr. Liatos worked as a Senior Associate for Gefinor USA, Inc., a private equity firm. From 1995 to 1997, Mr. Liatos worked as a Senior Associate at RJR Nabisco, Inc. in Financial Reporting and Consolidations. From 1992 to 1995, Mr. Liatos served as an auditor for Richard A. Eisner & Company, LLP. Mr. Liatos earned a B.S. in Business Administration from the Citadel. Mr. Liatos’ business executive knowledge and experience qualify him to serve on our board of directors.
Steven Rychnovsky, PhD has served as Kintara’s vice president, research and development since August 19, 2020. He previously served as Adgero’s Vice President of Operations and Product Development since 2016, and has held identical positions with Adgero since 2012. Dr. Rychnovsky is a co-founder of Adgero and has experience in all aspects of the photodynamic therapy (“PDT”) developed by Miravant Medical Technologies, and its wholly-owned subsidiaries, a former public pharmaceutical and research development company (collectively, “Miravant”), and, since 2012, Dr. Rychnovsky has worked with Dr. Pilkiewicz to develop Adgero’s business strategy and plans for commercialization of the REM-001 Therapy product, consisting of three parts, the laser light source, the light delivery device and the drug REM-001 (collectively, the “REM-001 Therapy”). From 2008 to 2012 Dr. Rychnovsky served as a consultant to St. Cloud Investments where his role was maintaining the Miravant assets and identifying a party to license or purchase those assets and pursue commercial development. In 2012, Dr. Rychnovsky was a co-founder of Endocole, LLC, a medical device company. He worked with Endocole from 2012 to 2015, where he focused on raising initial grant financing and worked in the development and preclinical testing of its proof-of-concept device and was a co-inventor of Endocole, LLC’s key intellectual property. EndoCole has completed its initial preclinical studies and is currently raising private funding to initiate a clinical study. From 2008 to 2012, Dr. Rychnovsky was a Senior Research Physicist at Sotera Defense Solutions, Inc., a Naval Research Laboratory optical nanotechnology group focused on applied research in optical materials and devices. From 2003 to 2008, Dr. Rychnovsky served as the Cardiovascular Program Manager at Miravant, where he invented key elements of Miravant’s cardiovascular technology. Dr. Rychnovsky also served as the Director of Systems and Engineering at Miravant where he managed the team responsible for development of Miravant’s PDT light delivery technology. During his time at Miravant, Dr. Rychnovsky was involved in new product development for its cancer, ophthalmology and cardiovascular programs, including clinical development of REM-001 and related PDT technology. Dr. Rychnovsky earned a B.S. in electrical engineering from Iowa State University, an M.S. in electrical engineering from the University of Minnesota, and has a PhD in photonics from the University of Iowa.
Robert J. Toth, Jr., MBA has served as a director of Kintara since August 20, 2013 and serves as Chair of Kintara’s Compensation Committee. Since 2005, Mr. Toth has primarily been managing his personal investment portfolio. From 2004-2005, Mr. Toth served as a consulting analyst to Narragansett Asset Management, a New York-based healthcare-focused hedge fund, where he advised the firm on biotechnology investments. From 2001-2003, he was the Senior Portfolio Manager for San Francisco-based EGM Capital’s Medical Technology hedge fund, where he was responsible for managing and maintaining a dedicated medical technology portfolio. Mr. Toth began his Wall Street career in 1996 as an Equity Research Associate for Vector Securities International, a healthcare-focused brokerage firm. From 1997-1999 he served as Senior Biotechnology Analyst. He joined Prudential Securities as Senior Vice President and Biotechnology Analyst where he served from 1999-2001 following Prudential’s acquisition of Vector. His responsibilities included the analysis of commercial, clinical and scientific fundamentals of oncology and genomics-based biotechnology companies on behalf of institutional investors. Mr. Toth was named to the Wall Street Journal’s Allstar List for stock picking in 1999. Mr. Toth received an MBA from the University of Washington and Bachelor of Science degrees in Biological Sciences and Biochemistry from California Polytechnic State University, San Luis Obispo. Mr. Toth’s financial and biotechnology industry knowledge and experience quality him to serve on our board of directors.
99
Laura Johnson has served as a director of Kintara since June 26, 2020. Ms. Johnson currently serves as the President and Chief Executive Officer of Next Generation Clinical Research, a contract research organization that Ms. Johnson founded in 1999. Additionally, Ms. Johnson is the President and Chief Executive Officer of Eufaeria Biosciences, Inc., a development biotechnology company that she founded in 2016. Ms. Johnson is also a founder and former member of the board of directors of SB Bancorp, Inc., a financial holding company, and Settlers Bank, Inc., a Wisconsin chartered business bank. In addition, Ms. Johnson serves as a member of the board of directors of La Jolla Pharmaceutical Company (Nasdaq: LJPC), a biopharmaceutical company, since 2013, Odonate Therapeutics (Nasdaq: ODT), a biopharmaceutical company, since 2018, Harmony Hill Farm Sanctuary since 2019 and Agrace HospiceCare from 2013 to 2016. In 2008 and 2010, she was honored as a biotechnology entrepreneur by the national organization, Women in Bio, and in 2008 received the Rising Star Award by the Wisconsin Biotech and Medical Device Association. Most recently, she was the recipient of the Wisconsin Biohealth Business Award at the BioForward Annual Biohealth Summit in October 2019. Ms. Johnson holds a nursing degree from The University of the State of New York-Albany. Ms. Johnson’s biotechnology industry and executive knowledge and experience qualify her to serve on our board of directors.
Keith Murphy has served as a director of director of Kintara since August 19, 2020. He served as a director of Adgero since August 2017. Adgero since August 2017. Mr. Murphy is Chairman, CEO and a founder of Viscient Bio, Inc., a biotech therapeutics company at the forefront of 3D human tissue disease modeling. Mr. Murphy previously was a founder and Chairman Emeritus of and served as the President, Chief Executive Officer of Organovo Holdings, Inc. from July 2007 through April 2017 and served as the Chairman of the board of directors from July 2007 through August 2017. Mr. Murphy previously served at Alkermes, Inc. (NASDAQ: ALKS), a biotechnology company, from July 1993 to July 1997, where he played a role on the development team for their first approved product, Nutropin (hGH) Depot. He moved to Amgen, Inc. (NASDAQ: AMGN) from August 1997 through July 2007. At Amgen, he held roles of increasing responsibility including Global Operations Leader for the osteoporosis/bone cancer drug Prolia/Xgeva (denosumab), the development of which involved several indications across multiple global Phase 3 studies. He holds a BS in Chemical Engineering from the Massachusetts Institute of Technology and is an alumnus of the UCLA Anderson School of Management. He sits on the board of directors of the California Life Sciences Association (CLSA). Mr. Murphy’s technical, operational, and extensive public capital markets experience qualify him to serve on our board of directors.
Our chief executive and chief financial officers are full-time employees and devote 100% of their business time to us. Our consulting agreement with Dr. Brown does not specify the amount of time Dr. Brown is required to devote to us, but does require that Dr. Brown provide us with the full benefit of his knowledge, expertise and ingenuity, and prohibits Dr. Brown from engaging in any business, enterprise or activity contrary to or that would detract from our business.
Our directors are appointed for a one-year term to hold office until the next annual general meeting of our stockholders or until removed from office in accordance with our bylaws and the provisions of the Nevada Revised Statutes.
Our officers are appointed by our board of directors and serve at its pleasure.
Involvement in Certain Legal Proceedings
To our knowledge, our directors and executive officers have not been involved in any of the following events during the past ten years:
|
|
1. |
any bankruptcy petition filed by or against such person or any business of which such person was a general partner or executive officer either at the time of the bankruptcy or within two years prior to that time; |
|
|
2. |
any conviction in a criminal proceeding or being subject to a pending criminal proceeding (excluding traffic violations and other minor offenses); |
|
|
3. |
being subject to any order, judgment, or decree, not subsequently reversed, suspended or vacated, of any court of competent jurisdiction, permanently or temporarily enjoining him from or otherwise limiting his involvement in any type of business, securities or banking activities or to be associated with any person practicing in banking or securities activities; |
|
|
4. |
being subject to any order, judgment or decree, not subsequently reversed, suspended or vacated, of any Federal or State authority barring, suspending or otherwise limiting for more than 60 days the right to engage in any activity described in paragraph (3) above, or to be associated with persons engaged in any such activity; |
|
|
5. |
being found by a court of competent jurisdiction in a civil action, the SEC or the Commodity Futures Trading Commission to have violated a Federal or state securities or commodities law, and the judgment has not been reversed, suspended, or vacated; |
100
|
|
6. |
being subject of, or a party to, any Federal or state judicial or administrative order, judgment decree, or finding, not subsequently reversed, suspended or vacated, relating to an alleged violation of (i) any Federal or state securities or commodities law or regulation, (ii) any law or regulation respecting financial institutions or insurance companies including, but not limited to, a temporary or permanent injunction, order of disgorgement or restitution, civil money penalty or temporary or permanent cease-and-desist order, or removal or prohibition order, or (iii) any law or regulation prohibiting mail or wire fraud or fraud in connection with any business entity; or |
|
|
7. |
being subject of or party to any sanction or order, not subsequently reversed, suspended, or vacated, of any self-regulatory organization, any registered entity or any equivalent exchange, association, entity or organization that has disciplinary authority over its members or persons associated with a member. |
Board Committees
The board of directors has formed an Audit Committee, which currently consists of Robert E. Hoffman, Chair, Robert Toth, Laura Johnson, and Keith Murphy all of whom are independent (as that term is defined under the Nasdaq Marketplace Rules) and financially literate (as such qualification is interpreted by the board of directors in its business judgment). In addition, our board of directors has determined that Mr. Hoffman qualifies as an audit committee financial expert within the meaning of SEC regulations and The NASDAQ Marketplace Rules.
The board of directors has also formed a Nominating and Corporate Governance Committee which consists of Laura Johnson, Chair, Robert Toth, and Keith Murphy. The Nominating and Corporate Governance Committee assists the board of directors in fulfilling its oversight responsibilities relating to corporate governance practices and policies.
In addition, the board of directors has formed a Compensation Committee which consists of Robert Toth, Chair, Keith Murphy, and Robert E. Hoffman. The Compensation Committee assists the board of directors in fulfilling its oversight responsibilities relating to compensation matters, including compensation of the directors and our senior management and the administration of our compensation plans.
Nomination of Directors
The Nominating and Corporate Governance Committee of the board of directors assesses potential candidates to fill perceived needs on the board of directors for required skills, expertise, independence and other factors. The Nominating and Corporate Governance Committee consists of independent directors only.
Orientation and Continuing Education
New members of the board of directors are provided with sufficient information to ensure that they are familiarized with us, our policies, and the mandates of the board of directors. Members of the board of directors are encouraged to communicate with management, legal counsel and, where applicable, our auditors and technical consultants to keep themselves current with industry developments and applicable legal, accounting and regulatory changes.
Board Leadership Structure and Role in Risk Oversight
Robert E. Hoffman serves as the chairman of our board of directors. Saiid Zarrabian serves as our Chief Executive Officer and President. We have not adopted a formal policy on whether the Chief Executive Officer and Chairman positions should be separated.
Our board of directors is primarily responsible for overseeing our risk management processes. The board of directors receives and reviews periodic reports from management, auditors, legal counsel, and others, as considered appropriate regarding our assessment of risks. The board of directors focuses on the most significant risks facing us and our general risk management strategy, and also ensures that risks undertaken by us are consistent with the board’s appetite for risk. While the board of directors oversees our risk management, management is responsible for the day-to-day risk management processes. We believe this division of responsibilities is the most effective approach for addressing the risks we face and that our board leadership structure supports this approach.
Code of Ethics
We have adopted a Code of Ethics and Business Conduct that applies to all of our executive officers, financial and accounting officers, our directors, our financial managers and all of our employees. Our board of directors is committed to a high standard of corporate governance practices and, through its oversight role, encourages and promotes a culture of ethical business conduct. A copy of our Code of Ethics and Business Conduct is posted under the “Investors” tab under Corporate Governance on our website, which is located at www.kintara.com.
101
Assessments
The board of directors assesses, on an ongoing basis, its overall performance and that of its committees in order to determine whether they are performing effectively. The board of directors also assesses, on an ongoing basis, the effectiveness and contribution of each of our directors, having regard to the competencies and skills each director is expected to bring to the board of directors.
Item 11. Executive Compensation.
Our board of directors has formed a Compensation Committee. The Compensation Committee is responsible for reviewing and approving management compensation, including salaries, bonuses, and equity compensation. We seek to provide competitive compensation arrangements that attract and retain key talent necessary to achieve our business objectives. At our 2018 annual meeting of stockholders, stockholders voted, on an advisory, non-binding basis, to approve the compensation paid to the company’s named executive officers, as disclosed in the proxy statement for the 2018 annual meeting. Our stockholders also voted, on an advisory, non-binding basis, that such votes on named executive officer compensation should be held every three years. The next advisory, non-binding vote to approve named executive officer compensation is expected to occur in connection with the 2021 annual meeting of stockholders.
Summary Compensation Table
The following table presents information regarding the total compensation awarded to, earned by, or paid to our Chief Executive Officer and the two most highly-compensated executive officers (other than the Chief Executive Officer) who were serving as executive officers as of June 30, 2020 and June 30, 2019 for services rendered in all capacities to us for the years ended June 30, 2020 and June 30, 2019. These individuals are our Named Executive Officers for 2020.
|
Name and Principal Position |
|
Period |
|
Salary (US$) |
|
|
Bonus Awards (US$) |
|
|
Equity Awards (US$) |
|
|
Total (US$) |
|
||||
|
Saiid Zarrabian, President and CEO |
|
Year Ended June 30, 2020 |
|
470,000(1) |
|
|
|
352,500 |
|
|
|
231,976 |
|
|
|
1,054,476 |
|
|
|
|
|
Year Ended June 30, 2019 |
|
|
470,000 |
|
|
|
165,665 |
|
|
|
— |
|
|
|
635,665 |
|
|
Dennis Brown, PhD, Chief Scientific Officer |
|
Year Ended June 30, 2020 |
|
200,000(2) |
|
|
|
— |
|
|
|
50,688 |
|
|
|
250,688 |
|
|
|
|
|
Year Ended June 30, 2019 |
|
|
200,000 |
|
|
|
— |
|
|
|
— |
|
|
|
200,000 |
|
|
Scott Praill, Chief Financial Officer |
|
Year Ended June 30, 2020 |
|
240,000(3) |
|
|
|
126,000 |
|
|
|
54,929 |
|
|
|
420,929 |
|
|
|
|
|
Year Ended June 30, 2019 |
|
|
220,000 |
|
|
|
52,250 |
|
|
|
30,627 |
|
|
|
302,877 |
|
|
(1) |
On July 7, 2017, Mr. Zarrabian was elected to the board of directors. On November 3, 2017, he was appointed interim chief executive officer and on January 1, 2018 he was also appointed interim president. On May 21, 2018, we entered into an employment agreement with Mr. Zarrabian pursuant to which Mr. Zarrabian was appointed as our permanent president and chief executive officer. Under the agreement, Mr. Zarrabian will receive an annual base salary of $470,000 and will be eligible to receive a fiscal year target bonus of up to 50% of base salary (which may be adjusted by the board of directors to up to 60% of base salary based on overachievement of bonus targets or other performance criteria). In September 2020, the Compensation Committee of the Board of Directors approved an additional bonus in the amount of $70.500 for performance during fiscal 2020, which amount is included in the $352,500. Any bonus earned for a fiscal year will be payable in cash, but the board of directors may pay up to 50% of the bonus, as well as any bonus in excess of 50% of base salary, in the form of stock options granted under the 2017 Plan (or any successor plan). The bonus for our fiscal year ended June 30, 2019 was based on the period from the effective date of the agreement (May 21, 2018) through June 30, 2019. The employment agreement may be terminated by us with or without cause (as defined therein). In the event we terminate the employment agreement without cause, we will be required to pay Mr. Zarrabian continued payment of his base salary for 12 months, a prorated bonus for the year of termination based on performance through the date of termination, an additional six months of vesting credit for any outstanding options, and continued health coverage during the severance period. In the event that an involuntary termination occurs during a period beginning sixty days before a definitive corporate transaction agreement is entered into that would result in a change in control (as defined therein), or within twelve months following a change in control, the severance period will increase to eighteen months’ severance, Mr. Zarrabian will receive 100% of his target bonus, and his options will be fully vested. |
102
During the fiscal year ended June 30, 2020, Mr. Zarrabian was granted stock options. On September 5, 2019 he was granted 457,650 stock options that are exercisable at $0.61 per share until September 5, 2029. Of the stock options granted, 241,438 were shares issuable upon the exercise of stock options which were subject to stockholder approval of the increase in the number of shares authorized for issuance under the 2017 Plan. On June 26, 2020 at our annual meeting of stockholders, the proposal to increase the number of shares authorized for issuance under the 2017 Plan was approved and the 241,438 stock options were issued. Mr. Zarrabian’s bonus for the fiscal year ended June 30, 2020 was $352,500.
|
(2) |
On January 1, 2015, we entered into a consulting agreement with Dr. Dennis Brown, our chief scientific officer. Subsequent to this agreement, it has been amended and is now renewed on an annual basis. Under the most recent renewal, Dr. Brown will continue to serve as our chief scientific officer until December 31, 2020, which period may be extended in accordance with the terms of the agreement. We will pay Dr. Brown an annual consulting fee of $200,000. During fiscal years 2020 and 2019, we paid Dr. Brown a consulting fee of $200,000. We may also pay to Dr. Brown a bonus and incentive compensation as determined at the discretion of the board of directors. The consulting agreement with Dr. Brown does not specify the amount of time Dr. Brown is required to devote to us, but does require that Dr. Brown provide us with the full benefit of his knowledge, expertise and ingenuity, and prohibits Dr. Brown from engaging in any business, enterprise or activity contrary to or that would detract from our business. |
During the fiscal year ended June 30, 2020, Dr. Brown was granted stock options. On September 5, 2019 he was granted 100,000 stock options that are exercisable at $0.61 per share until September 5, 2029. In addition, on November 12, 2019 he was granted 250,000 stock options that are exercisable at $0.735 until November 12, 2029. Of the stock options granted on September 5, 2019, 52,756 stock options and the 250,000 stock options granted on November 12, 2019 were shares issuable upon the exercise of stock options which were subject to stockholder approval of the increase in the number of shares authorized for issuance under the 2017 Plan. On June 26, 2020 at our annual meeting of stockholders, the proposal to increase the number of shares authorized for issuance under the 2017 Plan was approved and the 52,756 and 250,000 stock options, respectively, were issued.
|
(3) |
On February 9, 2017, we entered into an employment agreement with Scott Praill, our chief financial officer. Pursuant to the employment agreement, Mr. Praill will continue to serve as our chief financial officer for an indefinite period until termination of the employment agreement in accordance with its terms. We will pay Mr. Praill an annual base salary of $200,000 (which may be adjusted on an annual basis in the discretion of the board of directors) and Mr. Praill will also be eligible to participate in any bonus plan and long-term incentive plan established for our senior executives. The employment agreement may be terminated by us with or without cause (as defined therein). In the event we terminate the employment agreement without cause, we will be required to pay Mr. Praill, any accrued and unpaid base salary, plus an amount equal to 12 months of Mr. Praill’s base salary plus one additional month’s base salary for each completed year of service, up to 18 months’ base salary. On November 8, 2018, Mr. Praill was granted 10,000 stock options that are exercisable at $6.099 until November 8, 2028 for total compensation expense of $30,627. |
During the fiscal year ended June 30, 2020, Mr. Praill was granted stock options. On September 5, 2019 he was granted 108,366 stock options that are exercisable at $0.61 per share until September 5, 2029. Of the stock options granted, 57,170 were shares issuable upon the exercise of stock options which were subject to stockholder approval of the increase in the number of shares authorized for issuance under the 2017 Plan. On June 26, 2020 at our annual meeting of stockholders, the proposal to increase the number of shares authorized for issuance under the 2017 Plan was approved and the 57,170 stock options were issued. Mr. Praill’s bonus for the fiscal year ended June 30, 2020 was $126,000.
103
Outstanding Equity Awards at Fiscal Year-End
The following table sets forth outstanding equity awards to our named executive officers as of June 30, 2020, reflecting the one-for-ten reverse stock split that occurred on May 8, 2019.
|
|
Option awards |
|
|
Stock awards |
|
|||||||||||||||||||||
|
Name |
|
Number of securities underlying unexercised options (#) Exercisable |
|
|
Number of securities underlying unexercised options (#) un-exercisable |
|
|
Equity incentive plan awards: number of securities underlying unexercised unearned options (#) |
|
|
Option exercise price (US$) |
|
|
Option expiration date |
|
Equity incentive plan awards: Number of unearned shares, units or other rights that have not vested (#) |
|
|
Equity incentive plan awards: Market or payout value of unearned shares, units or other rights that have not vested ($) |
|
||||||
|
Saiid Zarrabian |
|
3,600(1) |
|
|
|
— |
|
|
|
— |
|
|
|
21.10 |
|
|
July 7, 2027 |
|
|
— |
|
|
|
— |
|
|
|
|
|
12,000(2) |
|
|
|
— |
|
|
|
— |
|
|
|
8.70 |
|
|
November 3, 2027 |
|
|
|
|
|
|
|
|
|
|
|
|
58,088(3) |
|
|
|
25,559 |
|
|
|
— |
|
|
|
9.825 |
|
|
May 21, 2028 |
|
|
|
|
|
|
|
|
|
|
|
|
114,414(7) |
|
|
|
343,236 |
|
|
|
— |
|
|
|
0.61 |
|
|
September 5, 2029 |
|
|
|
|
|
|
|
|
|
|
Dennis Brown, PhD |
|
|
3,750 |
|
|
|
— |
|
|
|
— |
|
|
20.00(5) |
|
|
February 1, 2022 |
|
|
— |
|
|
|
— |
|
|
|
|
|
|
8,750 |
|
|
|
— |
|
|
|
— |
|
|
|
42.00 |
|
|
August 15, 2023 |
|
|
|
|
|
|
|
|
|
|
|
9,360(4) |
|
|
|
— |
|
|
|
— |
|
|
|
49.50 |
|
|
February 17, 2027 |
|
|
|
|
|
|
|
|
|
|
|
|
25,001(7) |
|
|
|
74,999 |
|
|
|
— |
|
|
|
0.61 |
|
|
September 5, 2029 |
|
|
|
|
|
|
|
|
|
|
|
|
— (8) |
|
|
|
250,000 |
|
|
|
— |
|
|
|
0.735 |
|
|
November 12, 2029 |
|
|
|
|
|
|
|
|
|
|
Scott Praill |
|
|
1,250 |
|
|
|
— |
|
|
|
— |
|
|
20.00(5) |
|
|
February 1, 2022 |
|
|
— |
|
|
|
— |
|
|
|
|
|
|
8,750 |
|
|
|
— |
|
|
|
— |
|
|
|
42.00 |
|
|
August 15, 2023 |
|
|
|
|
|
|
|
|
|
|
|
3,740(4) |
|
|
|
— |
|
|
|
— |
|
|
|
49.50 |
|
|
February 17, 2027 |
|
|
|
|
|
|
|
|
|
|
|
|
5,278(6) |
|
|
|
4,722 |
|
|
|
— |
|
|
|
6.099 |
|
|
November 8, 2028 |
|
|
|
|
|
|
|
|
|
|
|
|
27,091(7) |
|
|
|
81,275 |
|
|
|
— |
|
|
|
0.61 |
|
|
September 5, 2029 |
|
|
|
|
|
|
|
|
|
|
(1) |
Stock options vest as to 1,200 on June 30, 2018, and 300 options vest each three months thereafter starting September 30, 2018. |
|
(2) |
Stock options vest pro rata monthly until full vesting on November 3, 2018. |
|
(3) |
Stock options vest as to 1/6th on November 21, 2018 with the remaining shares vesting in equal monthly installments over a period of 30 months commencing on December 21, 2018. |
|
(4) |
Stock options vest pro rata monthly until fully vesting on February 17, 2020. |
|
(5) |
Original exercise price was CDN $20.00. Price was amended to USD $20.00 on June 30, 2016. All other terms of the option grants remain unchanged. |
|
(6) |
Stock options vest as to 1/6th on May 8, 2019 with the remaining shares vesting in equal monthly installments over a period of 30 months commencing on June 8, 2019. |
|
(7) |
Stock options vest as to 1/6th on March 5, 2020 with the remaining shares vesting in equal monthly installments over a period of 30 months commencing on April 5, 2020. |
|
(8) |
Stock options vest based on the achievement of certain clinical milestones. |
Director Compensation
Director compensation is intended to provide an appropriate level of remuneration considering the responsibilities, time requirements and accountability of the directors.
104
The following table sets forth director compensation for the fiscal year ended June 30, 2020 (excluding compensation to our executive officers set forth in the summary compensation table above) paid by us, reflecting the one-for-ten reverse stock split that occurred on May 8, 2019.
|
Name |
|
Fees Earned or Paid in Cash ($)(1) |
|
|
Stock Awards ($) |
|
|
Option Awards ($)(2) |
|
|
Non-Equity Incentive Plan Compensation ($) |
|
|
Nonqualified Deferred Compensation Earnings ($) |
|
|
All Other Compensation ($) |
|
|
Total ($) |
|
|||||||
|
Robert E. Hoffman |
|
|
77,500 |
|
|
|
— |
|
|
|
35,915 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
113,415 |
|
|
John K. Bell(3) |
|
|
59,000 |
|
|
|
— |
|
|
|
35,915 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
94,915 |
|
|
Lynda Cranston |
|
|
47,500 |
|
|
|
— |
|
|
|
35,915 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
83,415 |
|
|
Napoleone Ferrara, MD |
|
|
49,000 |
|
|
|
— |
|
|
|
35,915 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
84,915 |
|
|
Robert J, Toth, Jr. |
|
|
57,500 |
|
|
|
— |
|
|
|
35,915 |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
93,415 |
|
|
Laura Johnson(4) |
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
(1) |
For our fiscal year ended June 30, 2020, our directors were paid a $40,000 annual retainer, an additional annual retainer for chairing a committee, a retainer for being a member of a committee, and the chairman of the board was paid an additional annual retainer of $25,000. |
|
(2) |
On September 5, 2019, independent directors were granted 75,000 stock options exercisable at $0.61 per share until September 5, 2029. The options vest pro rata over one year from the date of grant. Of the stock options granted, 39,567 for each independent director were shares issuable upon the exercise of stock options which were subject to stockholder approval of the increase in the number of shares authorized for issuance under the 2017 Plan. On June 26, 2020 at our annual meeting of stockholders, the proposal to increase the number of shares authorized for issuance under the 2017 Plan was approved and the 39,567 stock options for each independent director were issued. |
|
(3) |
Mr. Bell did not stand for re-election at our annual meeting of stockholders held on June 26, 2020. As a result, he forfeited any unvested stock options as of June 26, 2020. |
|
(4) |
Ms. Johnson was elected to the board of directors at our annual meeting of stockholders held June 26, 2020. |
Risk Management
We do not believe risks arising from its compensation policies and practices for its employees are reasonably likely to have a material adverse effect on us.
105
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The following table sets forth certain information, as of September 15, 2020, with respect to the beneficial ownership of the outstanding common stock, reflecting our one-for-ten reverse stock split occurring on May 8, 2019, by (i) any holder of more than five (5%) percent; (ii) each of our executive officers and directors; and (iii) our directors and executive officers as a group. Except as otherwise indicated, each of the stockholders listed below has sole voting and investment power over the shares beneficially owned.
|
Name of Beneficial Owner (1) |
|
Common Stock Beneficially Owned |
|
Percentage of Common Stock(2) |
|
||||
|
Directors and Officers |
|
|
|
|
|
|
|
|
|
|
Saiid Zarrabian |
|
|
267,051 |
|
(3) |
|
|
1.1 |
% |
|
Dennis Brown, PhD |
|
|
123,387 |
|
(4) |
|
* |
|
|
|
Scott Praill |
|
|
72,210 |
|
(5) |
|
* |
|
|
|
John Liatos |
|
|
196,750 |
|
(6) |
|
|
1.0 |
% |
|
Keith Murphy |
|
|
181,010 |
|
(7) |
|
* |
|
|
|
Robert E. Hoffman |
|
|
82,000 |
|
(8) |
|
* |
|
|
|
Robert J. Toth, Jr. |
|
|
87,139 |
|
(9) |
|
* |
|
|
|
Laura Johnson |
|
|
— |
|
|
|
|
— |
|
|
All officers and directors as a group (8 persons) |
|
|
1,009,547 |
|
|
|
|
4.3 |
% |
|
5% Holders |
|
|
|
|
|
|
|
|
|
|
Adam Stern |
|
|
1,653,970 |
|
(10) |
|
|
6.94 |
% |
|
Estate of Frank Pilkiewicz |
|
|
2,308,213 |
|
(11) |
|
|
9.8 |
% |
|
* |
Less than 1% |
|
(1) |
Except as otherwise indicated, the address of each beneficial owner is c/o Kintara Therapeutics, Inc., 12707 High Bluff Dr., Suite 200, San Diego, CA 92130. |
|
(2) |
Applicable percentage ownership is based on 23,543,892 shares of common stock outstanding as of September 15, 2020, together with securities exercisable or convertible into shares of common stock within 60 days of September 15, 2020 for each stockholder. Beneficial ownership is determined in accordance with the rules of the SEC and generally includes voting or investment power with respect to securities. Shares of common stock that are currently exercisable or exercisable within 60 days of September 15, 2020 are deemed to be beneficially owned by the person holding such securities for the purpose of computing the percentage of ownership of such person, but are not treated as outstanding for the purpose of computing the percentage ownership of any other person. |
|
(3) |
Includes 260,961 shares issuable upon the exercise of vested stock options. |
|
(4) |
Includes 53,750 shares held by Valent Technologies, LLC, 60,751 shares issuable upon exercise of vested stock options, 2,125 shares issuable upon exercise of warrants held by Dr. Brown, and 750 shares issuable upon the conversion of Series B Preferred Stock. |
|
(5) |
Includes 62,548 shares issuable upon exercise of vested stock options, 1,250 shares issuable upon exercise of warrants and 938 shares upon the conversion of Series B Preferred Stock. |
|
(6) |
Includes shares received upon the exchange of Adgero common shares. |
|
(7) |
Includes shares received upon the exchange of Adgero common shares and 58,236 shares issuable upon exercise of warrants. |
|
(8) |
Includes 82,000 shares issuable upon exercise of vested stock options. |
|
(9) |
Includes 85,600 shares issuable upon exercise of vested stock options and 325 shares issuable upon the conversion of Series B Preferred Stock. |
|
(10) |
The address of the stockholder is 810 Seventh Avenue, 22nd Floor, New York, NY 10019. Includes 80,104 shares held by A.K.S. Family Partners, L.P. (“AKSLP”) and 157 shares of Common Stock held by the AKS Family Foundation (“AKS”), (ii) 285,820 shares issuable upon the exercise of warrants, and (iii) 3,125 shares issuable upon the conversion of Series B Preferred Stock. Mr. Stern has voting and investment control of the securities held by AKSLP and AKS. Mr. Stern disclaims beneficial ownership of the securities held by AKSLP and AKS except as relates to this pecuniary interest in such securities. Does not include 258,996 shares underlying shares of Series C Preferred Stock or 744,600 shares of Common Stock underling Series C Preferred Stock issuable upon exercise of a warrant due to the beneficial ownership limitation of provision relating to the Series C Preferred Stock. |
106
|
(11) |
Includes (i) 75,223 shares held by his spouse, (ii) 9,715 shares issuable upon the exercise of warrants owned by his spouse, and (iii) 46,880 shares owned by his children. The address of Estate of Frank Pilkiewicz is Attn: Fox Rothchild, LLP, 997 Lenox Drive, Lawrenceville, NJ 08648. |
Securities Authorized for Issuance Under Equity Compensation Plans
The following table sets forth the aggregate information of our equity compensation plans in effect as of June 30, 2020:
|
Plan |
|
Number of securities to be issued upon exercise of outstanding options and rights |
|
|
Weighted- average exercise price of outstanding options and rights |
|
|
Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in first column |
|
|||
|
Equity compensation plans approved by security holders(1) |
|
|
1,394,964 |
|
|
$ |
1.35 |
|
|
|
720,801 |
|
|
Equity compensation plans not approved by security holders – Del Mar (BC) 2013 Amended and Restated Stock Option Plan |
|
|
164,235 |
|
|
$ |
32.25 |
|
|
|
— |
|
|
Totals |
|
|
1,559,199 |
|
|
$ |
4.61 |
|
|
|
720,801 |
|
|
(1) |
As approved by our stockholders at the annual meeting of stockholders held on April 11, 2018, on July 7, 2017, as amended on February 1, 2018, the board of directors approved the adoption of the 2017 Plan. The board of directors also approved a form of Performance Stock Unit Award Agreement to be used in connection with grants of performance stock units (“PSUs”) under the 2017 Plan. Under the 2017 Plan, as amended by an amendment approved by the board of directors on September 5, 2019, and our stockholders at its annual meeting of stockholders held on June 26, 2020, 2,280,000 shares of our common stock are reserved for issuance, less the number of shares of our common stock issued under the Legacy Plan or that are subject to grants of stock options made, or that may be made, under the Legacy Plan. A total of 164,235 shares of our common stock, net of forfeitures, have been issued under the Legacy Plan and/or are subject to outstanding stock options granted under the Legacy Plan, and a total of 1,394,964 shares of our common stock have been issued under the 2017 Plan and/or are subject to outstanding stock options granted under the 2017 Plan leaving a potential 720,801 shares of our common stock available for issuance under the Plan if all such options under the Legacy Plan were exercised and no new grants are made under the Legacy Plan. The maximum number of shares of our common stock with respect to which any one participant may be granted awards during any calendar year is 8% of our fully diluted shares of common stock on the date of grant (excluding the number of shares of our common stock issued under the 2017 Plan and/or the Legacy Plan or subject to outstanding awards granted under the 2017 Plan and/or the Legacy Plan). No award will be granted under the 2017 Plan on or after July 7, 2027, but awards granted prior to that date may extend beyond that date. Subsequent to June 30, 2020, the 2017 Plan was amended by an amendment approved by the board of directors on June 7, 2020, and our stockholders at the special meeting of stockholders held on August 14, 2020, to increase the number of shares reserved for issuance to 6,700,000 shares. |
Item 13. Certain Relationships and Related Transactions, and Director Independence.
Certain Relationships and Related Transactions
Valent Technologies LLC
On September 12, 2010, Del Mar (BC) entered into a Patent Assignment Agreement (the “Assignment”) with Valent Technologies LLC pursuant to which Valent assigned to Del Mar (BC) its rights to patent applications and the prototype drug product related to VAL-083. In accordance with the Assignment the consideration paid by Del Mar (BC) was $250,000 to acquire the prototype drug product. In accordance with the terms of the Assignment, Valent is entitled to receive a future royalty (in the single digits) on certain revenues derived from the development and commercialization of VAL-083. In the event that Del Mar (BC) terminates the agreement, Del Mar (BC) may be entitled to receive royalties from Valent’s subsequent development of VAL-083 depending on the development milestones Del Mar (BC) has achieved prior to the termination of the Assignment. The Assignment has a term (on a country-by-country basis), of the later of ten years or until patent rights covered by the Assignment no longer exist, subject to earlier termination in the event Del Mar (BC) breaches its payment obligations and fails to remedy such breach within 60 days, or if either party materially beaches any of its obligations and does not cure such breach within 30 days after receipt of notice thereof.
107
Pursuant to a loan agreement dated February 3, 2011, between Del Mar (BC) and Valent, Valent loaned Del Mar $250,000 for the purchase of the prototype drug product under the Assignment. The loan is unsecured, bears interest at 3% per year, and is payable on demand. Effective September 30, 2014, we entered into and closed an agreement with Valent to exchange its loan, including accrued interest to September 30, 2014, with Valent for 278,530 shares of our preferred stock. The preferred stock has an annual 3% dividend.
One of our officers, Dr. Dennis Brown, is a principal of Valent and as result Valent is a related party to us.
St. Cloud Investments, LLC
We acquired certain Miravant assets, including the REM-001 Therapy and the associated technology and intellectual property, through an asset purchase agreement with St. Cloud Investments, LLC (“St. Cloud”), dated November 26, 2012, as amended (the “St. Cloud Agreement”). St. Cloud was previously a Miravant creditor and acquired these Miravant assets pursuant to a foreclosure process St. Cloud completed under California law. Pursuant to the terms of the St. Cloud Agreement, we are obligated to make certain payments under the agreement. The amounts paid or owed under that agreement are as follows:
|
|
• |
Thirteen thousand dollars ($13,000) was paid to Steven Rychnovsky, PhD, our Vice President, Research and Development, upon the initial closing of an Adgero private placement conducted in 2016 (the “2016 Private Placement”). |
|
|
• |
Forty thousand dollars ($40,000) was paid to St. Cloud upon the initial closing of the 2016 Private Placement. |
|
|
• |
Fifty thousand dollars ($50,000) was paid to Steven Rychnovsky, PhD during the 2016 Private Placement, because the 2016 Private Placement was completed for an amount that exceeded four million dollars ($4,000,000). |
|
|
• |
Fifty thousand dollars ($50,000) was paid to St. Cloud during the 2016 Private Placement, because the 2016 Private Placement was completed for an amount that exceeded four million dollars ($4,000,000). |
|
|
• |
Upon the earlier of (i) a subsequent equity financing to take place after we conduct a Phase 2B clinical study in which fifty patients complete the study and their clinical data can be evaluated or (ii) the commencement of a clinical study intended to be used as a definitive study for market approval in any country, we are obligated to pay an aggregate amount of three hundred thousand dollars ($300,000) in cash or an equivalent amount of common stock, with two hundred forty thousand dollars ($240,000) to St. Cloud and sixty thousand dollars ($60,000) to Steven Rychnovsky, PhD. |
|
|
• |
Upon receipt of regulatory approval of REM-001 Therapy, we are obligated to pay an aggregate amount of seven hundred thousand dollars ($700,000) in cash or an equivalent amount of common stock, with five hundred and sixty thousand dollars ($560,000) to St. Cloud and one hundred forty thousand dollars ($140,000) to Steven Rychnovsky, PhD. |
With respect to the $300,000 and $700,000 potential milestone payments referenced above (each a “Milestone Payment”), if either such Milestone Payment becomes payable, and in the event we elect to pay either such Milestone Payment in shares of our common stock, the value of the common stock will equal the price per share of the most recent financing, or, if we are considered to be a publicly-traded company, the average of the closing price per share of our common stock over the twenty (20) trading days following the first public announcement of the applicable event described above.
In addition, we must pay to St. Cloud and Steven Rychnovsky, PhD, in the aggregate, a royalty fee of six percent (6%) of net sales during the royalty term on a country-by-country and product-by-product basis with St. Cloud receiving a royalty rate of four and eight tenths percent (4.8%) and Steven Rychnovsky, PhD, receiving a royalty of one and two tenths percent (1.2%). The royalty term for a product commences on the first commercial sale of the product, such as REM-001 Therapy, in any country, and the royalty fee must be paid within 30 days of each calendar quarter during which revenue is collected. The royalty term terminates on the later of (i) the invalidation, revocation, lapse or expiration of the last to expire valid claim on any patent acquired in the St. Cloud Agreement that would be infringed by the sale of the product in the country where the commercial sale takes place or (ii) the expiration of the period for which we hold exclusive marketing rights of the product in the country, if we were granted those rights under the St. Cloud Agreement.
One of our officers, Dr. Steven Rychnovsky, is entitled to receive payments and royalties under the St. Cloud Agreement.
Director Independence
Robert E. Hoffman, Robert J. Toth, Jr., Laura Johnson, and Keith Murphy are independent as that term is defined under the Nasdaq Marketplace Rules.
108
Item 14. Principal Accounting Fees and Services.
On July 31, 2019, Marcum LLP (“Marcum”), Certified Public Accountants, were appointed as our new auditors.
Ernst & Young LLP (“E&Y”), Chartered Professional Accountants, were our auditors until July 31, 2019.
The following is a summary of fees paid by us for professional services rendered by Marcum for the year ended June 20, 2020 and by E&Y for the year ended June 30, 2019.
|
|
|
Year Ended June 30, 2020 |
|
|
Year Ended June 30, 2019 |
|
||
|
Audit fees |
|
$ |
130,000 |
|
|
$ |
132,800 |
|
|
Audit related fees |
|
$ |
30,950 |
|
|
$ |
182,800 |
|
|
Tax fees |
|
$ |
— |
|
|
$ |
— |
|
|
All other fees |
|
$ |
— |
|
|
$ |
— |
|
|
Total fees |
|
$ |
160,950 |
|
|
$ |
315,600 |
|
Audit fees. Audit fees represent fees for professional services performed by Marcum or E&Y for the audit of our annual financial statements and the review of our quarterly financial statements, as well as services that are normally provided in connection with statutory and regulatory filings or engagements.
Audit-related fees. Audit-related fees represent fees for assurance and related services performed by Marcum or E&Y that are reasonably related to the performance of the audit or review of our financial statements.
Tax Fees. Neither Marcum nor E&Y has not performed any tax compliance services for us during the years ended June 30, 2020 or 2019.
All other fees. Neither Marcum nor E&Y received any other fees from us for the years ended June 30, 2020 or 2019.
In accordance with applicable laws, rules and regulations, our audit committee charter and pre-approval policies established by the audit committee require that the audit committee review in advance and pre-approve all audit and permitted non-audit fees for services provided to us by our independent registered public accounting firm. The services performed by, and the fees to be paid to Marcum and E&Y, in 2020 and 2019, respectively, were approved by the audit committee.
109
|
2.1 |
|
|
|
|
|
|
|
2.2†† |
|
|
|
|
|
|
|
3.1 |
|
|
|
|
|
|
|
3.2 |
|
|
|
|
|
|
|
3.3 |
|
|
|
|
|
|
|
3.4 |
|
|
|
|
|
|
|
3.5 |
|
|
|
|
|
|
|
3.6 |
|
|
|
|
|
|
|
3.7 |
|
|
|
|
|
|
|
3.8 |
|
|
|
|
|
|
|
3.9 |
|
|
|
|
|
|
|
3.10 |
|
|
|
|
|
|
|
3.11 |
|
|
|
|
|
|
|
3.12 |
|
|
|
|
|
|
|
3.13 |
|
|
|
|
|
|
|
3.14 |
|
|
|
|
|
|
|
3.15 |
|
|
|
|
|
|
|
3.16 |
|
|
|
|
|
|
|
3.17 |
|
|
|
|
|
|
110
|
4.1 |
|
|
|
|
|
|
|
4.2 |
|
|
|
|
|
|
|
4.3 |
|
|
|
|
|
|
|
4.4 |
|
|
|
|
|
|
|
4.5 |
|
|
|
|
|
|
|
4.6 |
|
|
|
|
|
|
|
4.7 |
|
|
|
|
|
|
|
4.8 |
|
|
|
|
|
|
|
4.9 |
|
|
|
|
|
|
|
4.10 |
|
|
|
|
|
|
|
4.11 |
|
|
|
|
|
|
|
4.12 |
|
|
|
|
|
|
|
4.13 |
|
|
|
|
|
|
|
4.14 |
|
|
|
|
|
|
|
4.15 |
|
|
|
|
|
|
|
4.16 |
|
|
|
|
|
|
|
10.1 |
|
|
|
|
|
|
|
10.2 |
|
|
|
|
|
|
|
10.3 |
|
|
|
|
|
|
|
10.4 |
|
|
|
|
|
|
|
10.5 |
|
|
|
|
|
|
111
|
10.6† |
|
|
|
|
|
|
|
10.7† |
|
|
|
|
|
|
|
10.8 |
|
|
|
|
|
|
|
10.9 |
|
|
|
|
|
|
|
10.10 |
|
|
|
|
|
|
|
10.11 |
|
|
|
|
|
|
|
10.12 |
|
|
|
|
|
|
|
10.13 |
|
|
|
|
|
|
|
10.14 |
|
|
|
|
|
|
|
10.15 |
|
|
|
|
|
|
|
10.16 |
|
|
|
|
|
|
|
10.17 |
|
|
|
|
|
|
|
10.18 |
|
|
|
|
|
|
|
10.19 |
|
|
|
|
|
|
|
10.20 |
|
|
|
|
|
|
|
10.21 |
|
|
|
|
|
|
|
10.22 |
|
|
|
|
|
|
|
10.23 |
|
|
|
|
|
|
112
|
10.24 |
|
|
|
|
|
|
|
10.25 |
|
|
|
|
|
|
|
10.26 |
|
Amendment to the 2017 Omnibus Equity Incentive Plan of Kintara Therapeutics, Inc.* |
|
|
|
|
|
16.1 |
|
|
|
|
|
|
|
16.2 |
|
|
|
|
|
|
|
21.1 |
|
|
|
|
|
|
|
23.1 |
|
|
|
|
|
|
|
23.2 |
|
|
|
|
|
|
|
31.1 |
|
|
|
|
|
|
|
31.2 |
|
|
|
|
|
|
|
32.1 |
|
|
|
|
|
|
|
32.2 |
|
|
|
|
|
|
|
EX-101.INS |
|
XBRL Instance Document * |
|
|
|
|
|
EX-101.SCH |
|
XBRL Taxonomy Extension Schema Document * |
|
|
|
|
|
EX-101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase * |
|
|
|
|
|
EX-101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase * |
|
|
|
|
|
EX-101.LAB |
|
XBRL Taxonomy Extension Labels Linkbase * |
|
|
|
|
|
EX-101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase * |
|
† |
Confidential treatment is requested for certain confidential portions of this exhibit pursuant to Rule 24b-2 under the Exchange Act. In accordance with Rule 24b-2, these confidential portions have been omitted from this exhibit and filed separately with the Commission. |
|
†† |
Schedule has been omitted pursuant to Item 601(a)(5) of Regulation S-K. The Company hereby undertakes to furnish copies of any of the omitted schedules upon request by the Securities and Exchange Commission. |
|
* |
Filed herewith |
|
** |
Furnished herewith |
None.
113
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
KINTARA THERAPEUTICS, INC. |
||
|
|
|
|
|
|
Dated: September 18, 2020 |
By: |
/s/ Saiid Zarrabian |
|
|
|
|
Name: |
Saiid Zarrabian |
|
|
|
Title: |
Chief Executive Officer |
|
Dated: September 18, 2020 |
By: |
/s/ Scott Praill |
|
|
|
|
Name: |
Scott Praill |
|
|
|
Title: |
Chief Financial Officer |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
SIGNATURE |
|
TITLE |
|
DATE |
|
|
|
|
|
|
|
/s/ Saiid Zarrabian |
|
Chief Executive Officer, Director |
|
September 18, 2020 |
|
Saiid Zarrabian |
|
(principal executive officer) |
|
|
|
|
|
|
|
|
|
/s/ Scott Praill |
|
Chief Financial Officer |
|
September 18, 2020 |
|
Scott Praill |
|
(principal financial and accounting officer) |
|
|
|
|
|
|
|
|
|
/s/ Dennis Brown |
|
Chief Scientific Officer |
|
September 18 2020 |
|
Dennis Brown |
|
|
|
|
|
|
|
|
|
|
|
/s/ John Liatos |
|
Director |
|
September 18, 2020 |
|
John Liatos |
|
|
|
|
|
|
|
|
|
|
|
/s/ Robert J. Toth |
|
Director |
|
September 18, 2020 |
|
Robert J. Toth |
|
|
|
|
|
|
|
|
|
|
|
/s/ Laura Johnson |
|
Director |
|
September 18, 2020 |
|
Laura Johnson |
|
|
|
|
|
|
|
|
|
|
|
/s/ Robert E. Hoffman |
|
Director |
|
September 18, 2020 |
|
Robert E. Hoffman |
|
|
|
|
|
|
|
|
|
|
|
/s/ Keith Murphy |
|
Director |
|
September 18, 2020 |
|
Keith Murphy |
|
|
|
|
114